Baseline chest radiograph obtained on admission for future comparison.
Admission chest radiograph obtained for baseline comparison; extensive chronic parenchymal changes from prior pneumonias limit detailed assessment.
X-ray obtained for outpatient specialist review; no acute abnormality noted.
Chest radiograph
Chest X-ray within normal limits.
No interval change since prior exam.
Heart size within normal limits.
Mild increase in bilateral lobar haziness compared with admission; recommend clinical correlation and laboratory evaluation.
Interval increase in bilateral infiltrates and consolidation, indicating pneumonia exacerbation.
Worsening bilateral infiltrates and consolidation consistent with progressive pneumonia.
No definitive change; slight increase in bilateral lobar haziness compared with the prior study, of uncertain significance; further clinical correlation and blood tests are recommended.
CXR is equivocal between possible consolidation and motion artifact. Clinical correlation required.
This chest radiograph was obtained for submission to a specialist for further evaluation.
Bowel gas pattern
Unremarkable bowel gas pattern.
No abnormal mass shadow or calcification identified.
Gas-filled central small-bowel loops.
Dilated bowel loops concerning for obstruction.
Distended colon with extensive stool burden, compatible with severe constipation or fecal impaction.
Mildly distended colon with minimal stool burden, consistent with mild constipation.
HFNC (M0046 for HFNC, MM400 for BiPAP)
Apply HFNC: 40 L/min@FiO2 0.30; keep SpO2>= 92 %
Start HFNC 60 L/min @ FiO2 40%; SpO2 ≥ 92%; reassess in 30 min
No significant fracture
No significant fracture seen.
L-tube
Upon its protruding into the oral cavity, insert a new 18Fr L-tube.
Upon its having protruded into the oral cavity, a new 18Fr L-tube was inserted.
Misc
Stitch-out of three simple sutures
Auscultation
Abdominal auscultation – normal
Normoactive bowel sounds in all four quadrants.
Abd auscultation: bowel sounds present and normoactive.
Written on May 21, 2025
Radiological Report Expressions
Auscultation and radiological assessments are pivotal in diagnosing various clinical conditions. The following tables provide a structured summary of radiological findings across different clinical scenarios.
Chest
Comparative Assessment
Clinical Scenario
Radiological Description
Baseline Radiograph
Upon admission, a baseline radiograph was obtained for comparative assessment against subsequent radiographic studies.
Changes Compared to Previous Exam
Compared to the previous examination, there is evidence of worsened lung infiltration and consolidation in bilateral lung fields, suggestive of an exacerbation of the underlying pneumonia process.
No interval changes detected; the X-ray appears within normal limits.
No remarkable interval change since the previous study.
No Admission Radiograph
X-ray not performed until discharge.
Admission X-ray not done before discharge.
Lungs
Clinical Scenario
Radiological Description
Normal Findings
No active lung lesions observed. Lungs are essentially clear.
Lungs appear clear with no abnormalities detected.
Infiltrates and Consolidation
Consolidation involving multiple lung lobes.
Worsened bilateral lung infiltrates and consolidation, consistent with an exacerbation of pneumonia.
Decreased consolidation/Ground-Glass Opacity (GGO) in bilateral lower lobes, indicative of improving pneumonia.
Chronic Pathology
Recurrent pneumonia suggested by chronic parenchymal lung pathology. Clinical correlation and ongoing observation are crucial for a definitive diagnosis.
Heart
Clinical Scenario
Radiological Description
Normal Findings
Heart size is within normal limits. No enlargement detected.
Abdomen
Bowel Gas Pattern
Clinical Scenario
Radiological Description
Normal Findings
No remarkable findings in the bowel gas pattern of the abdomen.
Obstruction Indicators
Gas-filled loops of small bowel observed in the central abdomen.
Dilated loops of bowel, suggestive of bowel obstruction.
Imaging reveals dilated bowel loops with some improvement in motility compared to the previous study on May 20th.
Constipation
Clinical Scenario
Radiological Description
Constipation
Abdominal X-ray reveals notable findings consistent with constipation.
The colon appears distended with significant gas accumulation, particularly in the sigmoid and descending colon.
Marked retention of feces throughout the large bowel, indicative of fecal impaction.
Prominent stool burden observed throughout the colon.
Additional Findings
Clinical Scenario
Radiological Description
Fractures
No significant fractures detected.
Mass Shadows or Calcifications
No abnormal mass shadows or calcifications observed.
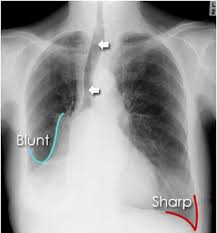
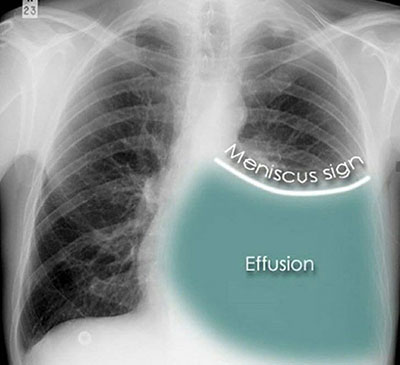
Pleural Effusion
Slightly increased amount of left pleural effusion.
Decreased right pleural effusion.
Written on December 2nd, 2024
Heart and Lung Auscultation Findings
Auscultation of the heart and lungs is a fundamental clinical skill essential for diagnosing various cardiopulmonary conditions. The following tables provide a concise yet comprehensive summary of auscultation findings for both the heart and lungs across different clinical scenarios.
Heart Auscultation Findings
Clinical Scenario
Auscultation Description
Normal Findings
S1 and S2 heart sounds audible with a regular rate and rhythm. No murmurs, rubs, or gallops detected.
Murmur Detected
Grade 3/6 systolic ejection murmur best heard at the left sternal border, radiating to the carotid arteries.
Gallop Rhythm (S3)
Presence of an S3 gallop, suggestive of volume overload.
Gallop Rhythm (S4)
Detection of an S4 gallop, indicative of decreased ventricular compliance.
Pericardial Rub
Audible pericardial friction rub, triphasic in nature, loudest during end-expiration.
Irregular Rhythm
Irregularly irregular rhythm with variable S1 intensity, consistent with atrial fibrillation.
Lung Auscultation Findings
Clinical Scenario
Auscultation Description
Normal Findings
Bilateral breath sounds clear and vesicular, with no adventitious sounds present.
Fine Crackles (Rales)
Presence of fine crackles at bilateral lung bases, consistent with pulmonary edema.
Coarse Crackles
Coarse crackles heard over the right lower lobe, suggestive of pneumonia.
Wheezing
Diffuse expiratory wheezing bilaterally, indicative of bronchospasm.
Rhonchi
Low-pitched rhonchi detected in the right lower lobe, with improvement following coughing.
Absent Breath Sounds
Absence of breath sounds over the left hemithorax, consistent with pneumothorax.
Audible pleural friction rub over the right mid-zone.
Diminished Breath Sounds
Breath sounds in the left lung are less distinct than in the right, making it more challenging to assess for pneumonia on the left side.
Pneumonia Specific Findings
Presence of localized coarse crackles and bronchial breath sounds in the affected lobe, possibly accompanied by increased tactile fremitus and egophony.
Written on December 2nd, 2024
Pharmacological Management of Cardiovascular Conditions
Receptor and Channel Mechanisms in the Cardiovascular System
The cardiovascular system is intricately regulated by receptors and ion channels that respond to neurotransmitters and pharmacological agents. Below is a comprehensive overview of alpha, beta, and dopaminergic receptors, as well as ion channels involved in cardiac function, along with associated medications.
Below is a detailed table summarizing the antiarrhythmic drug classes, their mechanisms, medications, indications, contraindications, elimination pathways, and common side effects.
Notes:
- Dosage Information: Specific dosing is patient-specific and should be determined by a healthcare professional.
- Pediatric Use: Some medications may have limited data in pediatric populations and require specialist consultation.
- Elimination Pathways: Understanding hepatic versus renal elimination is crucial for dose adjustments in organ impairment.
- Side Effects: Monitoring is essential to detect adverse effects early.
Key Points for Each Antiarrhythmic Class
Class I (Sodium Channel Blockers):
Ia: Quinidine, Procainamide—used for a wide range of arrhythmias but have significant side effects.
Ib: Lidocaine—primarily for acute ventricular arrhythmias, especially post-MI.
Ic:Flecainide—effective for atrial fibrillation; contraindicated in structural heart disease due to proarrhythmic risk.
Class II (Beta Blockers):
Reduce sympathetic stimulation; beneficial in tachyarrhythmias and preventing sudden cardiac death post-MI.
Class III (Potassium Channel Blockers):
Amiodarone is widely used due to its efficacy but requires monitoring for toxicity.
Sotalol also has beta-blocking properties.
Class IV (Calcium Channel Blockers):
Effective for supraventricular tachycardias; avoid in patients with heart failure with reduced ejection fraction.
Comparative Analysis of Dopamine vs. Norepinephrine
Dopamine and norepinephrine are both widely utilized vasopressors in critical care settings, employed to elevate blood pressure through distinct mechanisms and clinical applications. Understanding their specific modes of action and potential clinical impacts can aid in the judicious selection of these agents based on patient needs and underlying conditions.
(A) Dopamine
Mechanism of Action: Dopamine operates on various adrenergic and dopaminergic receptors depending on dosage. At lower doses (1–5 µg/kg/min), dopamine primarily activates dopaminergic receptors, promoting vasodilation in renal and mesenteric vessels. At intermediate doses (5–10 µg/kg/min), it acts on β1-adrenergic receptors, enhancing heart rate and contractility, thus improving cardiac output. High doses (>10 µg/kg/min) predominantly stimulate α1-adrenergic receptors, leading to vasoconstriction and an increase in systemic vascular resistance (SVR).
Clinical Use: Dopamine is frequently used in scenarios where both cardiac output and blood pressure require augmentation. Its β1 effects make it especially effective for patients with concurrent heart failure. However, dopamine's propensity to cause tachycardia and arrhythmias can limit its use, particularly among patients predisposed to these conditions.
(B) Norepinephrine
Mechanism of Action: Norepinephrine primarily engages α1-adrenergic receptors, producing strong vasoconstriction that elevates SVR and, consequently, blood pressure. Although norepinephrine also exhibits β1-adrenergic effects, which can modestly increase heart rate and cardiac contractility, its dominant action lies in regulating vascular tone.
Clinical Use: Often selected as a first-line treatment for hypotension, norepinephrine is especially favored in septic shock due to its potent vasoconstrictive capabilities. By predominantly influencing vascular tone, it raises blood pressure with a relatively lower effect on heart rate, rendering it advantageous for patients who may not tolerate elevated heart rates.
(C) Key Differences
Receptor Activity: Dopamine exhibits a dose-dependent profile, engaging dopaminergic, β1, and α1 receptors. In contrast, norepinephrine is primarily α1-adrenergic with some β1 activity.
Heart Rate Effects: Dopamine is more likely to induce an increase in heart rate, which may lead to tachyarrhythmias. Norepinephrine, by comparison, has a lesser impact on heart rate, making it a safer alternative for patients with existing tachycardia or susceptibility to arrhythmias.
Preferred Indications: Dopamine is often employed in cases necessitating enhanced cardiac output, as seen in heart failure patients. Norepinephrine is preferred in septic or distributive shock where its vasoconstrictive effect is critical to raising blood pressure.
Overall, while both agents serve as effective vasopressors, their distinctive receptor profiles and clinical implications guide their application in patient-specific contexts.
Written on October 16, 2024
Management of Hypotension with Dobutamine Infusion: Systolic vs. Diastolic Blood Pressure Monitoring
Hypotension necessitates prompt and effective management to ensure adequate organ perfusion and prevent organ dysfunction. Dobutamine hydrochloride (Inopan) is an inotropic agent frequently employed to enhance cardiac output in hypotensive patients. This document delineates strategies for managing hypotension with dobutamine infusion, emphasizing the roles of systolic blood pressure (SBP) and diastolic blood pressure (DBP) monitoring. Special considerations for elderly patients under hospice care and those presenting with wide pulse pressure are also discussed.
(A) Dobutamine Infusion for Hypotension
Prior to initiating therapy, it is imperative to dilute the desired dose of dobutamine appropriately. Specifically, 4 ampules of dobutamine hydrochloride (0.2 g/5 mL) should be mixed in a 500 cc normal saline (N/S) solution. The infusion rate is calculated in micrograms per kilogram per minute (mcg/kg/min), typically ranging from 2 to 20 mcg/kg/min. Commencing at a lower dose, approximately 2.5 mcg/kg/min, facilitates careful titration based on the patient's response.
(B) Infusion Rate Adjustments Based on Blood Pressure
Systolic Blood Pressure Monitoring
Blood Pressure Category
SBP (mmHg)
Initial Infusion Rate
Considerations
Mild Hypotension
90–100
2.5 mcg/kg/min
Monitor SBP closely; adjust infusion rate upwards if necessary
Moderate Hypotension
70–90
5–10 mcg/kg/min
Frequent SBP monitoring is crucial; titrate based on hemodynamic response
Severe Hypotension
<70
10–20 mcg/kg/min
Close monitoring required due to risks of tachyarrhythmias and increased myocardial oxygen demand
Improvement in BP
>100 (SBP)
Gradually taper
Aim for hemodynamic stability; adjust infusion rate downward
Persistent Low BP
As above
Increase within therapeutic range
Avoid excessive rates; monitor for side effects such as tachycardia or arrhythmias
Diastolic Blood Pressure Monitoring
Blood Pressure Category
DBP (mmHg)
Initial Infusion Rate
Considerations
Mildly Low DBP
50–60
2.5 mcg/kg/min
Avoid overcompensation; moderate rate increases may be needed
Moderately Low DBP
40–50
5–10 mcg/kg/min
Supports adequate diastolic pressure and coronary perfusion
Severely Low DBP
<40
10–20 mcg/kg/min
Rapid adjustments are critical due to risks of inadequate organ perfusion
DBP Improvement
>60
Gradually taper
Aim to maintain DBP in a range ensuring both systemic and coronary perfusion
Persistent Low DBP
As above
Increase within therapeutic range
Avoid excessive rates; monitor for side effects such as tachycardia or arrhythmias
(C) Systolic vs. Diastolic Blood Pressure Monitoring
Parameter
Systolic Blood Pressure (SBP)
Diastolic Blood Pressure (DBP)
Advantages
- Broad indicator of systemic perfusion pressure
- Easier to monitor and commonly used in acute settings
- Directly assesses severity of hypotension or shock
- Critical for assessing coronary blood flow during diastole
- Reflects vascular tone and resistance
Best Use Cases
- Acute management where the primary concern is organ perfusion
- Patients without significant coronary artery disease
- Patients with ischemic heart disease or at risk of myocardial ischemia
- Situations involving vasodilation or decreased vascular tone
Disadvantages
- May overlook diastolic hypotension affecting coronary perfusion
- Focusing solely on DBP might underestimate systemic perfusion needs
- Potential for over-intervention in hospice settings
Combined Monitoring Approach: Monitoring both SBP and DBP provides a comprehensive understanding of the patient’s hemodynamic status:
Balancing Perfusion Needs: Ensures both systemic and coronary perfusion are maintained.
Optimizing Therapy: Allows precise titration of dobutamine to support cardiac and systemic function effectively.
(D) Special Considerations: Wide Pulse Pressure
A wide pulse pressure (difference >60 mmHg between SBP and DBP) often indicates decreased arterial compliance, common in elderly patients.
Implications
Factor
Details
Aortic Stiffness and Arteriosclerosis
Leads to elevated SBP and low DBP, reflecting decreased arterial compliance.
Increased Cardiovascular Risk
Associated with higher risks of heart failure and stroke.
Recommended Approach
Parameter
Target Range
Considerations
Moderate SBP Control
120–140 mmHg
Reduces cardiac strain and risk of stroke or heart failure.
Maintain Adequate DBP
≥50 mmHg
Prevents myocardial ischemia and ensures adequate coronary perfusion.
(E) Dobutamine Infusion Rate Guidelines
Blood Pressure Category
SBP (mmHg)
DBP (mmHg)
Initial Infusion Rate
Considerations
Mild Hypotension
90–100
50–60
2.5 mcg/kg/min
Monitor BP; titrate upwards if needed
Moderate Hypotension
70–90
40–50
5–10 mcg/kg/min
Frequent BP monitoring; adjust based on hemodynamic response
Severe Hypotension
<70
<40
10–20 mcg/kg/min
Close monitoring required; watch for tachyarrhythmias and increased myocardial oxygen demand
Improvement in BP
>100 (SBP)
>60 (DBP)
Gradually taper
Aim for hemodynamic stability; adjust infusion rate downward
Persistent Low BP
As above
As above
Increase within therapeutic range
Avoid excessive rates; monitor for side effects such as tachycardia or arrhythmias
Note: This document is intended for informational purposes and should be utilized in conjunction with clinical judgment and individual patient considerations.
Written on October 22, 2024
Pulmonology
Nebulized Medications for Respiratory Management
Nebulized medications are essential in the management of various respiratory conditions, including asthma, chronic obstructive pulmonary disease (COPD), cystic fibrosis, and bronchitis. By delivering drugs directly to the lungs, nebulization enables rapid absorption and targeted action, making it an efficient approach for relieving bronchospasm, reducing inflammation, and improving airflow. Below is a comprehensive outline of the primary categories of nebulized medications, including mechanisms, effects, dosage guidelines, and an in-depth comparison of two prominent bronchodilators, Ventolin (albuterol) and Atrovent (ipratropium bromide).
(A) Bronchodilators
A-1) Beta-2 Agonists
A-1-i) Short-Acting Beta-2 Agonists (SABA)
Examples: Albuterol (Salbutamol), Levalbuterol
Mechanism of Action: These medications stimulate beta-2 adrenergic receptors in bronchial smooth muscle, leading to muscle relaxation and bronchodilation.
Effects: They provide rapid relief from bronchoconstriction, improve airflow, and ease breathing. Typically used for acute exacerbations of asthma or COPD.
Dosage:
Albuterol (Salbutamol): 2.5 mg to 5 mg every 4–6 hours as needed.
Levalbuterol: 0.31 mg to 1.25 mg, generally every 6–8 hours.
A-1-ii) Long-Acting Beta-2 Agonists (LABA)
Examples: Formoterol, Arformoterol
Mechanism of Action: Long-acting agents stimulate beta-2 receptors and provide prolonged bronchodilation, typically lasting 12 hours or more.
Effects: Suitable for maintaining stable bronchodilation and reducing the frequency of exacerbations, especially for chronic management of COPD or severe asthma.
Dosage:
Formoterol: 20 mcg twice daily.
Arformoterol: 15 mcg twice daily.
A-2) Anticholinergics
A-2-i) Short-Acting Muscarinic Antagonists (SAMA)
Examples: Ipratropium Bromide
Mechanism of Action: SAMAs block muscarinic receptors in airway smooth muscle, preventing acetylcholine-induced bronchoconstriction.
Effects: Provide short-term bronchodilation, often used in conjunction with SABAs for enhanced efficacy in acute COPD exacerbations.
Dosage: Typically 0.5 mg every 4–6 hours as needed.
A-2-ii) Long-Acting Muscarinic Antagonists (LAMA)
Examples: Tiotropium
Mechanism of Action: LAMAs provide prolonged muscarinic receptor blockade, resulting in sustained bronchodilation.
Effects: Suitable for long-term COPD management, reducing exacerbation frequency and improving lung function.
Dosage: Tiotropium is typically administered once daily in inhalation forms; nebulized forms are less commonly used.
Aspect
Ventolin (Albuterol/Salbutamol)
Atrovent (Ipratropium Bromide)
Drug Class
Beta-2 Adrenergic Agonist (Short-Acting)
Anticholinergic/Antimuscarinic (Short-Acting)
Mechanism of Action
Stimulates beta-2 adrenergic receptors in the bronchial smooth muscle, leading to rapid muscle relaxation and bronchodilation.
Blocks muscarinic receptors in the bronchial smooth muscle, preventing acetylcholine-induced bronchoconstriction.
Onset of Action
Rapid, typically within 5–15 minutes
Moderate, usually within 15–30 minutes
Duration of Action
Approximately 4–6 hours, short-acting
Also around 4–6 hours, short-acting
Indications
Primarily used for acute relief of bronchospasm in asthma and COPD, especially effective during exacerbations.
Primarily used in COPD management; occasionally in asthma. Effective when combined with beta-agonists for enhanced bronchodilation.
Dosage (Nebulized)
Generally 2.5 mg every 4–6 hours as needed
Typically 0.5 mg every 4–6 hours as needed
Primary Effects
Provides quick relief from acute bronchospasm, reduces wheezing, and improves airflow.
Reduces airway resistance, provides bronchodilation, and decreases mucus secretion.
Common Side Effects
Tremor, nervousness, tachycardia, and palpitations
Dry mouth, cough, headache, and occasionally blurred vision.
Unique Considerations
Considered the frontline rescue treatment for acute asthma exacerbations due to its rapid onset and beta-2 agonist effect.
Often preferred in COPD due to its ability to reduce mucus secretion, and it complements beta-2 agonists like Ventolin effectively.
Ventolin is widely used as a rescue medication for acute asthma attacks, with its rapid onset of action making it highly effective for immediate bronchodilation.
Atrovent is advantageous in COPD management, where its anticholinergic effects can provide additional bronchodilation and reduce mucus production. When combined with beta-2 agonists such as Ventolin, Atrovent enhances bronchodilation by leveraging different pathways, offering superior symptom relief than either drug alone.
2. Corticosteroids
Examples: Budesonide, Methylprednisolone
Mechanism of Action: Corticosteroids reduce airway inflammation by inhibiting inflammatory cytokines and immune cell activity.
Effects: Reduce airway edema, mucus production, and hyperresponsiveness, leading to improved lung function over time. They are indicated for long-term control in chronic respiratory diseases.
Dosage:
Budesonide: 0.5 mg to 1 mg twice daily.
Methylprednisolone: Not typically used for nebulization; preferred systemically for acute needs.
Mechanism of Action: Mucolytics reduce the viscosity of mucus by breaking down its molecular structure, making clearance from the airways easier.
Effects: Aid in mucus clearance, reducing airway obstruction and facilitating breathing. Primarily beneficial for thick mucus-associated conditions, such as cystic fibrosis and chronic bronchitis.
Dosage:
Acetylcysteine: 3–5 mL of 10–20% solution, administered 3–4 times daily.
Dornase Alfa: 2.5 mg once daily for cystic fibrosis patients; some cases benefit from twice-daily administration.
4. Antibiotics
Examples: Tobramycin, Aztreonam, Colistin
Mechanism of Action: Inhaled antibiotics provide high-concentration delivery directly to the lungs, targeting chronic bacterial infections such as Pseudomonas in cystic fibrosis or bronchiectasis.
Tobramycin: 300 mg twice daily, often in 28-day cycles.
Aztreonam: 75 mg three times daily, also in 28-day cycles.
Colistin: 75–150 mg twice daily, depending on infection severity and patient tolerance.
- written on October 29th, 2024 -
Tuberculosis
TB, MDR-TB, and XDR-TB
Tuberculosis (TB), Multidrug-Resistant Tuberculosis (MDR-TB), and Extensively Drug-Resistant Tuberculosis (XDR-TB) represent significant clinical and public health challenges. These conditions, defined by their varying resistance profiles, require specific diagnostic and therapeutic approaches. A detailed exploration follows, including the antibiotics used, potential side effects, and precise criteria for determining a cure.
Tuberculosis (TB)
Definition
Tuberculosis is a bacterial infection caused by Mycobacterium tuberculosis. It primarily affects the lungs (pulmonary TB) but may also involve other organs (extrapulmonary TB).
Diagnosis
Clinical Presentation: Chronic cough, hemoptysis, fever, night sweats, fatigue, and weight loss.
Radiological Imaging: Chest X-rays or CT scans for structural abnormalities.
Latent TB Tests: Tuberculin Skin Test (TST) or Interferon-Gamma Release Assays (IGRA).
Treatment
Standard First-Line Drugs:
Isoniazid (INH): Inhibits mycolic acid synthesis.
Side effects: Hepatotoxicity, peripheral neuropathy (prevented with pyridoxine).
Rifampin (RIF): Inhibits RNA synthesis.
Side effects: Hepatotoxicity, orange discoloration of bodily fluids, drug interactions.
Pyrazinamide (PZA): Effective in acidic environments, targeting dormant bacilli.
Side effects: Hepatotoxicity, hyperuricemia, arthralgia.
Ethambutol (EMB): Inhibits cell wall synthesis.
Side effects: Optic neuritis (dose-dependent, reversible).
Regimen:
2 months of intensive phase: INH, RIF, PZA, EMB.
4 months of continuation phase: INH, RIF.
Cure Criteria
Negative sputum cultures at the end of treatment.
Consecutive negative cultures (minimum of two) taken at least one month apart.
Resolution of clinical and radiological abnormalities.
Multidrug-Resistant Tuberculosis (MDR-TB)
Definition
MDR-TB is caused by strains of Mycobacterium tuberculosis resistant to at least Isoniazid (INH) and Rifampin (RIF), the two most potent first-line drugs.
Diagnosis
Rapid Molecular Diagnostics:
GeneXpert MTB/RIF for rifampin resistance detection.
Drug Susceptibility Testing (DST):
Testing for INH and other first-line drugs.
Line Probe Assays (LPAs):
Detect specific mutations conferring drug resistance.
Side effects: Myelosuppression, peripheral neuropathy.
Regimen:
Combination of at least four effective second-line drugs.
Duration: 18-24 months, tailored to patient response and drug tolerance.
Cure Criteria
Consecutive negative cultures (minimum of three) taken at least one month apart during the final six months of treatment.
Absence of clinical and radiological evidence of active disease.
No recurrence within a specified follow-up period (typically 12 months).
Extensively Drug-Resistant Tuberculosis (XDR-TB)
Definition
XDR-TB is an advanced form of MDR-TB with additional resistance to at least one fluoroquinolone and one injectable second-line drug.
Diagnosis
Comprehensive Drug Susceptibility Testing (DST):
Includes both first-line and second-line drugs.
Whole Genome Sequencing (WGS):
Identifies specific resistance mutations.
Phenotypic Culture Testing:
Confirms resistance patterns observed in molecular assays.
Treatment
Advanced Regimens:
Novel Drugs: Bedaquiline (BDQ), Delamanid (DLM).
Repurposed Drugs: Clofazimine, Carbapenems (e.g., Meropenem) with Amoxicillin-Clavulanate.
Adjunctive Therapy: High-dose Vitamin D for immune modulation.
Regimen:
Individualized combination of novel, repurposed, and second-line drugs.
Duration: Often exceeds 24 months, adjusted based on patient response and drug tolerance.
Cure Criteria
Minimum of six consecutive negative cultures taken at monthly intervals during the final phase of treatment.
Continuous clinical improvement with radiological stability or resolution.
No evidence of relapse within two years of completing therapy.
Aspect
TB
MDR-TB
XDR-TB
Definition
Drug-sensitive M. tuberculosis.
Resistant to INH and RIF.
MDR-TB with additional resistance to fluoroquinolones and injectables.
Diagnosis
Sputum smear, culture, NAATs.
DST, GeneXpert, LPAs.
Comprehensive DST, whole genome sequencing.
Treatment
INH, RIF, PZA, EMB for 6 months.
Second-line drugs for 18-24 months.
Tailored regimens with novel and repurposed drugs for >24 months.
Drugs
INH, RIF, PZA, EMB.
Fluoroquinolones, injectables, BDQ, LZD.
BDQ, DLM, Clofazimine, Carbapenems.
Side Effects
Hepatotoxicity, neuropathy, optic neuritis.
Nephrotoxicity, QT prolongation, ototoxicity.
Similar to MDR-TB with added complexity (e.g., increased risk of QT prolongation).
Cure Criteria
Two negative cultures at end of therapy.
Three negative cultures in final 6 months.
Six negative cultures with two-year follow-up.
This refined and detailed presentation serves as a comprehensive resource for understanding and managing TB, MDR-TB, and XDR-TB, emphasizing precision and thoroughness. Further refinements are welcome to ensure clarity and utility.
- written on November 15th, 2024 -
Analysis and Diagnostic Protocol for Tuberculosis (Written February 13, 2025)
This document provides an integrated analysis of key diagnostic tests for tuberculosis (TB), including their pricing, sensitivity, specificity, and clinical purpose. The tests reviewed include the Acid-Fast Bacilli (AFB) stain, AFB culture, chest X-ray, and the Interferon-Gamma Release Assay (IGRA). In addition, an algorithmic protocol is proposed to guide the diagnostic pathway, facilitating early detection and appropriate management of TB cases.
Test
Sensitivity
Specificity
Purpose
AFB Stain
~30–60% (variable by sample)
~95%
Rapid screening for TB by detecting acid-fast bacilli in sputum specimens.
AFB Culture
~70–90%
Nearly 100%
Confirmatory diagnosis; enables drug susceptibility testing and pathogen identification.
Chest X-ray
~80–90%
~50–70%
Imaging to identify pulmonary abnormalities suggestive of TB; used as an initial screening tool.
IGRA (Interferon-Gamma Release Assay)
~75–90%
~95–100%
Detection of latent TB infection by assessing immune response to TB-specific antigens.
Diagnostic Algorithm for Tuberculosis
The following algorithm outlines a systematic approach to TB diagnosis, incorporating the diagnostic tests discussed above. This protocol is designed to optimize test selection based on initial clinical assessment, radiological findings, and laboratory results.
Initial Clinical Evaluation
Assess patient history, symptoms (e.g., chronic cough, weight loss, fever, night sweats), and risk factors.
Primary Screening
Perform an AFB Stain on sputum specimen.
If Positive: Proceed to confirmatory testing (AFB Culture).
If Negative but Suspicion Remains High: Proceed to Chest X-ray.
Radiological Assessment
Conduct a Chest X-ray to detect pulmonary abnormalities.
If Abnormal Findings Suggestive of TB: Proceed to AFB Culture for confirmatory diagnosis.
If Chest X-ray is Non-diagnostic: Consider IGRA to evaluate latent TB infection.
Confirmatory Testing
Perform AFB Culture to definitively diagnose TB and assess drug susceptibility.
If Positive Culture: Confirm TB diagnosis and initiate appropriate treatment.
If Negative Culture with Persistent Clinical Suspicion: Consider additional tests, including IGRA and clinical re-evaluation.
Latent TB Infection Assessment
Use IGRA when there is a history of Bacille Calmette-Guérin (BCG) vaccination or for screening of contacts or individuals with suspected latent TB.
Antibiotic Classifications, Mechanisms, Examples, and Clinical Application
Antibiotics encompass a wide range of drug classes, each with unique mechanisms of action, spectrums of activity, and clinical uses. Understanding these classifications, along with their abbreviations, common brand names, recommended dosages for specific conditions, and considerations for antibiotic susceptibility testing (AST), is crucial for effective and responsible antibiotic therapy. Below is a refined and detailed overview of key antibiotic classes, their characteristics, and clinical application guidelines.
1. Beta-Lactam Antibiotics
1.1 Beta-Lactamase Inhibitors
Beta-lactamase inhibitors are compounds that inhibit bacterial beta-lactamases, enzymes that degrade beta-lactam antibiotics. They are typically combined with beta-lactam antibiotics to enhance their effectiveness against resistant bacteria.
Mechanism:
These inhibitors bind irreversibly to the active site of beta-lactamase enzymes, preventing them from breaking down the antibiotic.
Note: Beta-lactamase inhibitor combinations often require AST to tailor the therapy effectively.
1.2 Penicillins
Penicillins are among the earliest classes of antibiotics, effective against a wide range of bacteria including some Gram-positive and Gram-negative organisms.
Mechanism:
Penicillins inhibit cell wall synthesis by binding to penicillin-binding proteins (PBPs), preventing the cross-linking of the peptidoglycan cell wall.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Penicillin G (PEN G)
Pfizerpen
Syphilis, endocarditis, pneumonia, meningitis caused by susceptible organisms
For pneumonia (IV): 2-4 million units every 4-6 hours
Cephalosporins are beta-lactam antibiotics subdivided into generations, each with varying spectrums of activity. They are used to treat a wide range of infections, from skin infections to more serious hospital-acquired infections.
Mechanism:
Similar to penicillins, cephalosporins inhibit cell wall synthesis by binding to PBPs.
For community-acquired pneumonia (IV): 600 mg every 12 hours
Yes
IV
1.4 Carbapenems
Carbapenems are broad-spectrum beta-lactam antibiotics typically reserved for severe or high-risk bacterial infections, including those resistant to other beta-lactams.
Mechanism:
Carbapenems bind to PBPs, inhibiting the final transpeptidation step of cell wall synthesis.
For hospital-acquired pneumonia (IV): 500 mg every 8 hours
No
IV
1.5 Monobactams
Monobactams are beta-lactam antibiotics effective primarily against Gram-negative bacteria and are often used in patients with penicillin allergies.
Mechanism:
Monobactams inhibit bacterial cell wall synthesis by binding selectively to PBPs of Gram-negative bacteria.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Aztreonam (AZT)
Azactam
Pseudomonas infections, UTIs, pneumonia
For pneumonia (IV): 1-2 g every 6-8 hours
Yes
IV, IM
2. Glycopeptides
Glycopeptides are antibiotics that target Gram-positive bacteria, including multi-resistant strains such as Methicillin-Resistant Staphylococcus aureus (MRSA).
Mechanism:
Glycopeptides inhibit cell wall synthesis by binding to the D-alanyl-D-alanine terminus of cell wall precursors, preventing peptidoglycan synthesis.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Vancomycin (VAN)
Vancocin, Firvanq
MRSA infections, severe C. difficile infection
For MRSA pneumonia (IV): 15-20 mg/kg every 8-12 hours
No
IV, Oral
Teicoplanin (TEC)
Targocid
MRSA infections, endocarditis, osteomyelitis
For MRSA infections (IV): 6 mg/kg every 12 hours for 3 doses, then daily
Yes
IV, IM
Dalbavancin (DAL)
Dalvance
Acute bacterial skin and skin structure infections (ABSSSI) caused by Gram-positive organisms
Single-dose regimen (IV): 1500 mg x1
Yes
IV
Oritavancin (ORI)
Orbactiv
ABSSSI caused by Gram-positive organisms
Single-dose regimen (IV): 1200 mg x1
Yes
IV
Note: Serum drug levels for vancomycin are often monitored to ensure therapeutic levels and reduce toxicity risk.
3. Aminoglycosides
Aminoglycosides are broad-spectrum antibiotics, particularly effective against Gram-negative bacteria and often used in combination with other antibiotics for severe infections such as sepsis.
Mechanism:
Aminoglycosides bind to the 30S subunit of bacterial ribosomes, causing misreading of mRNA and inhibition of protein synthesis.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Gentamicin (GEN)
Garamycin
Sepsis, endocarditis (in combination), UTIs
For sepsis (IV): Loading dose of 2 mg/kg, then 1-1.7 mg/kg every 8 hours
Yes
IV, IM
Amikacin (AMK)
Amikin
Severe Gram-negative infections, sepsis
For sepsis (IV/IM): 15 mg/kg once daily or divided doses
Yes
IV, IM
Tobramycin (TOB)
Nebcin
Pseudomonas infections, severe UTIs
For Pseudomonas pneumonia (IV): 5-7 mg/kg once daily
Yes
IV, IM
Streptomycin (SM)
—
Tuberculosis (in combination therapy)
For tuberculosis (IM): 15 mg/kg once daily
Yes
IM
Neomycin (NEO)
Neo-Fradin, Mycifradin
Bowel decontamination, topical infections
Topical or oral only
Yes
Oral, Topical
Note: Aminoglycosides require careful monitoring of serum levels due to nephrotoxicity and ototoxicity risk.
4. Tetracyclines
Tetracyclines are broad-spectrum antibiotics effective against various bacterial infections and some atypical organisms. They are used for conditions like acne, pneumonia, and certain STDs.
Mechanism:
Tetracyclines bind to the 30S ribosomal subunit, inhibiting the attachment of aminoacyl-tRNA to the mRNA-ribosome complex, thereby preventing protein synthesis.
Complicated skin and intra-abdominal infections, community-acquired pneumonia
For complicated infections (IV): 100 mg loading dose, then 50 mg every 12 hours
Yes
IV
Note: Tetracyclines can cause photosensitivity and are contraindicated in children under 8 years and pregnant women.
5. Oxazolidinones
Oxazolidinones are synthetic antibiotics primarily used for treating Gram-positive bacterial infections, including those resistant to other antibiotics, such as MRSA and VRE (Vancomycin-Resistant Enterococci).
Mechanism:
Oxazolidinones inhibit the initiation of bacterial protein synthesis by binding to the 50S ribosomal subunit, preventing the formation of the 70S initiation complex.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Linezolid (LNZ)
Zyvox
MRSA pneumonia, VRE infections, skin infections
For MRSA pneumonia (oral/IV): 600 mg every 12 hours
Yes
Oral, IV
Tedizolid (TZD)
Sivextro
Acute bacterial skin and skin structure infections (ABSSSI) caused by Gram-positive organisms
For ABSSSI (oral/IV): 200 mg once daily for 6 days
Yes
Oral, IV
Note: Linezolid and tedizolid can cause hematological side effects; monitoring blood counts is recommended during long-term use.
6. Streptogramins
Streptogramins are antibiotics used particularly against Gram-positive bacteria, including multi-resistant strains like MRSA and VRE.
Mechanism:
Streptogramins bind to distinct sites on the 50S ribosomal subunit, inhibiting protein synthesis. Quinupristin binds to a site, resulting in a conformational change in the ribosome that enhances the binding of dalfopristin.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Quinupristin/Dalfopristin (Q/D)
Synercid
VRE infections (E. faecium), MRSA infections, complicated skin infections
For VRE infections (IV): 7.5 mg/kg every 8 hours
Yes
IV
Note: Quinupristin/dalfopristin is not active against Enterococcus faecalis. Adjustments may be needed based on AST results.
7. Chloramphenicol
Chloramphenicol is a broad-spectrum antibiotic effective against a variety of bacteria. However, its use is limited due to serious side effects such as aplastic anemia.
Mechanism:
Chloramphenicol inhibits bacterial protein synthesis by binding to the 50S ribosomal subunit and preventing peptide bond formation.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Chloramphenicol (CAP)
Chloromycetin, Viceton
Typhoid fever, meningitis, rickettsial infections
For serious infections (IV): 50-100 mg/kg/day in divided doses every 6 hours
Yes
IV, Oral
Note: Chloramphenicol requires regular monitoring of blood counts due to the risk of aplastic anemia.
8. Macrolides
Macrolides are antibiotics effective primarily against Gram-positive bacteria and some Gram-negative bacteria. They are often used for respiratory infections, skin infections, and sexually transmitted infections.
Mechanism:
Macrolides bind to the 50S subunit of bacterial ribosomes, inhibiting the translocation step of protein synthesis.
For C. difficile infection (oral): 200 mg every 12 hours for 10 days
Yes
Oral
Note: Macrolides have drug-drug interactions due to CYP450 metabolism. AST is not always required for typical pathogens unless resistance is suspected.
9. Lincosamides
Lincosamides are antibiotics effective mainly against Gram-positive cocci and anaerobes. They are used in various infections including skin and soft tissue infections, and anaerobic infections.
Mechanism:
Lincosamides bind to the 50S subunit of the bacterial ribosome, inhibiting protein synthesis by blocking the translocation step.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Clindamycin (CLI)
Cleocin, Dalacin
Anaerobic infections, skin infections, pneumonia
For MRSA skin infections (oral): 300-450 mg every 6 hours
Yes
Oral, IV, IM
Lincomycin (LNM)
Lincocin
Similar to clindamycin but less commonly used
For serious infections (IM/IV): 600 mg every 8-12 hours
Yes
IV, IM
Note: Clindamycin is known to cause C. difficile-associated diarrhea; AST recommended to ensure susceptibility.
10. Fluoroquinolones
Fluoroquinolones are broad-spectrum antibiotics effective against a variety of Gram-positive and Gram-negative organisms. They are widely used for respiratory infections, UTIs, and abdominal infections.
Mechanism:
Fluoroquinolones inhibit bacterial DNA gyrase and topoisomerase IV, enzymes essential for DNA replication and transcription.
Note: Fluoroquinolones can cause QT prolongation and tendon rupture. AST is typically recommended for severe infections or resistant organisms.
11. Quinolones (Non-Fluorinated)
Quinolones are an older class of antibiotics, primarily effective against Gram-negative bacteria. They have largely been replaced by fluoroquinolones with broader spectrums and better pharmacokinetics.
Mechanism:
Quinolones inhibit bacterial DNA replication by targeting DNA gyrase (topoisomerase II).
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Nalidixic Acid (NAL)
Wintomylon
Uncomplicated UTIs
For UTIs (oral): 1 g every 6 hours
Yes
Oral
Note: Nalidixic acid is of historical interest and is rarely used due to bacterial resistance and availability of better agents.
12. Sulfonamides
Sulfonamides are synthetic bacteriostatic antibiotics effective against a wide range of Gram-positive and Gram-negative bacteria. They are frequently used in combination with dihydrofolate reductase inhibitors.
Mechanism:
Sulfonamides inhibit dihydropteroate synthase, an enzyme involved in folate synthesis, thus preventing bacterial growth.
Antibiotic
Common Combination
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Sulfamethoxazole (SMX) combined with Trimethoprim as Co-Trimoxazole (TMP-SMX)
For pneumonia (oral/IV): 15-20 mg/kg/day (based on TMP) in divided doses every 6-8 hours
No
Oral, IV
Sulfadiazine (SDZ)
Combined with pyrimethamine
—
Toxoplasmosis
For toxoplasmosis (oral): 1000 mg four times daily in combination with pyrimethamine
Yes
Oral
Note: Adequate hydration is needed to prevent crystalluria; monitoring for hypersensitivity reactions is important.
13. Dihydrofolate Reductase (DHFR) Inhibitors
DHFR inhibitors are often combined with sulfonamides to achieve a synergistic bactericidal effect by inhibiting successive steps in folate synthesis.
Mechanism:
These agents inhibit dihydrofolate reductase, an enzyme required for folate synthesis and bacterial DNA replication.
Antibiotic
Common Combinations
Indications
Dosage Recommendations
AST
Route
Trimethoprim (TMP)
Combined with sulfamethoxazole as co-trimoxazole
UTIs, PCP, MRSA skin infections
See TMP-SMX dosage recommendations in sulfonamides section
No
Oral, IV
Pyrimethamine (PYR)
Combined with sulfadiazine
Toxoplasmosis, pneumocystis pneumonia in combination therapy
For toxoplasmosis (oral): 200 mg loading dose, then 50-75 mg daily in combination with sulfadiazine
Yes
Oral
Note: Folate supplementation may be required during long-term therapy to prevent hematological side effects.
14. Nitroimidazoles
Nitroimidazoles are effective primarily against anaerobic bacteria and protozoa. They are commonly used for infections like C. difficile colitis, intra-abdominal infections, and gynecological infections.
Mechanism:
Nitroimidazoles cause DNA strand breakage and inhibit nucleic acid synthesis in anaerobic organisms by interacting with their DNA.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Metronidazole (MTZ)
Flagyl, Metrogyl
Anaerobic infections, C. difficile colitis, trichomoniasis
For C. difficile infection (oral): 500 mg three times daily for 10-14 days
Yes
Oral, IV
Tinidazole (TND)
Tindamax
Trichomoniasis, bacterial vaginosis, giardiasis
For trichomoniasis (oral): 2 g single dose
Yes
Oral
Note: Patients should avoid alcohol during and 48 hours after treatment with nitroimidazoles due to a disulfiram-like reaction.
15. Rifamycins
Rifamycins are a class of antibiotics with potent activity against Mycobacterium tuberculosis and other organisms. They are commonly used in tuberculosis treatment regimens and for prophylaxis against certain infections.
Mechanism:
Rifamycins inhibit bacterial DNA-dependent RNA polymerase by binding to the β-subunit, preventing RNA synthesis.
Antibiotic
Common Brand Names
Indications
Dosage Recommendations
AST
Route
Rifampin (RIF)
Rifadin, Rimactane
Tuberculosis, meningococcal prophylaxis
For tuberculosis (oral/IV): 10 mg/kg (up to 600 mg) once daily
Yes
Oral, IV
Rifabutin (RBT)
Mycobutin
TB in HIV patients, Mycobacterium avium complex prophylaxis
For traveler's diarrhea (oral): 200 mg three times daily for 3 days
No
Oral
Note: Rifamycins have strong inducing effects on the cytochrome P450 system, leading to drug-drug interactions.
Conclusion
Each antibiotic class has distinct mechanisms of action, spectrums of activity, and clinical uses. Knowledge of these classes, along with representative antibiotics, their acronyms, commonly known brand names, recommended dosages for specific infections, and requirements for antibiotic susceptibility testing (AST), is crucial for effective treatment.
This comprehensive overview aims to guide clinical decision-making by providing detailed information on the selection and use of various antibiotic agents. Continual updates and refinements are encouraged to keep pace with the evolving landscape of antibiotic development and resistance patterns, ensuring that practitioners are well-equipped to choose the most appropriate therapy for their patients.
Note: All dosage recommendations are general guidelines and may vary based on patient factors such as age, weight, renal function, and severity of infection. Appropriate AST, therapeutic drug monitoring, and clinical judgment should be applied when selecting and dosing antibiotics.
IV Antibiotics Reference Guide
This table offers physicians a comprehensive platform to review essential information about IV antibiotics, including dosage, concentration, recommended dosage for standard adult pneumonia, and contraindications/interactions.
Medication
Class
Supplied As
pH
Concentration (mg/mL)
Rec Dosage for Standard Adult Pneumonia
Contraindications/Interactions
Ampicillin/Sulbactam (Unasyn)
Penicillin/Beta-lactamase Inhibitor
mg
7 - 8
-
1,500 - 3,000 mg IV every 6 hours
Avoid in penicillin allergy; monitor for rash. Effective against beta-lactamase producing organisms; monitor renal function. Applicable for MRAB.
Piperacillin / Tazobactam (Zosyn)
Penicillin / Beta-lactamase inhibitor
mg
5.5
-
4,500 - 6,000 mg IV every 6 hours
Avoid in penicillin allergy; monitor renal function.
Cefepime
Cephalosporin
mg
4.5
-
1,000 - 2,000 mg IV every 8-12 hours
Caution in renal impairment; neurotoxicity.
Ceftazidime / Avibactam (Avycaz)
Cephalosporin / Beta-lactamase Inhibitor
mg
5.5 - 6.5
-
2,000 mg IV every 8 hours
Avoid in severe penicillin or cephalosporin allergies; monitor renal function. Applicable for CRE.
Ceftaroline (Teflaro)
Cephalosporin
mg
6.0
-
600 mg IV every 12 hours
Avoid in cephalosporin or penicillin allergies; risk of allergic reactions with beta-lactam antibiotics. Applicable for MRSA.
Ceftolozane / Tazobactam (Zerbaxa)
Cephalosporin / Beta-lactamase Inhibitor
mg
5.5 - 6.0
-
1,500 mg IV every 8 hours
Avoid in cephalosporin or beta-lactamase inhibitor allergies; monitor renal function, risk of nephrotoxicity. Applicable for MRPA.
Cefiderocol (Fetroja)
Siderophore Cephalosporin
mg
5.0 - 7.0
-
2,000 mg IV every 8 hours
Avoid in cephalosporin allergy; monitor renal function, risk of kidney damage in renal impairment. Applicable for CRE, MRPA, MRAB.
Vancomycin
Glycopeptide
mg
2.5 - 4.5
-
15-20 mg/kg IV every 8-12 hours
Nephrotoxicity; "Red man syndrome"; Requires TDM. Effective against MRSA but not VRE.
Teicoplanin (Targocid)
Glycopeptide
mg
7.2
-
400 mg loading dose, then 200 mg IV every 24 hours
Ototoxicity; nephrotoxicity. Requires loading dose for optimal levels. Alternative for MRSA and can be considered for VRE with caution.
Daptomycin (Cubicin)
Lipopeptide
mg
7.4
-
500 mg IV every 24 hours
Avoid in daptomycin allergy; risk of muscle damage (rhabdomyolysis), especially with statins. Monitor CPK levels. Applicable for MRSA, VRE.
Ciprofloxacin
Fluoroquinolone
mg
3.9
-
400 mg
Tendon rupture risk; avoid in myasthenia gravis.
Levofloxacin
Fluoroquinolone
mg
4.5 - 5
-
500 - 750 mg
Tendon rupture risk; QT prolongation.
Metronidazole (Flagyl)
Nitroimidazole
mg
5.5 - 6
-
500 mg IV every 8 hours (as adjunctive therapy for PMC)
Avoid alcohol; disulfiram-like reaction. Used as adjunctive therapy for pneumonia requiring anaerobic coverage (PMC).
Avoid in beta-lactam allergy; seizure risk in CNS disorders. Caution with drugs that lower seizure threshold. Applicable for CRE, MRPA, MRAB.
Meropenem
Carbapenem
mg
7.3
-
500 - 1,000 mg IV every 8 hours
Seizure risk; adjust dose in renal impairment. Effective against MRPA but not against CRE.
Meropenem/Vaborbactam (Vabomere)
Carbapenem/Beta-lactamase Inhibitor
mg
7.3
-
4,000 mg IV every 8 hours
Avoid in beta-lactam allergy; risk of seizures, especially in CNS disorders. Monitor renal function. Applicable for CRE.
Ertapenem (Invanz)
Carbapenem
mg
7.5
-
1,000 mg IV once daily
Not for pediatric use; seizure risk.
Gentamicin
Aminoglycoside
mg/mL
4.0
40
3 - 5 mg/kg/day IV divided into 2-3 doses
Ototoxicity and nephrotoxicity; IM permissible.
Amikacin
Aminoglycoside
mg/mL
3.5
250
15 mg/kg/day IV once or divided doses
Ototoxicity and nephrotoxicity; IM permissible. Effective against MRPA;
Tigecycline (Tygacil)
Glycylcycline
mg
4.5 - 5
-
100 - 100 mg IV every 12 hours
Not for children; may increase mortality. Effective against VRE and some MRSA strains; not recommended as monotherapy for pneumonia.
Colistin (Polymyxin E)
Polymyxin
mg
6 - 8
-
2.5 - 5 mg/kg IV loading dose, then 1.25 - 2.5 mg/kg IV every 12 hours
Nephrotoxicity; neurotoxicity. Last-resort option for CRE, MRPA, and MRAB. Requires careful dosing and monitoring of renal function. Effective against MRSA in combination therapy; use Linezolid or Vancomycin as first-line for MRSA.
Linezolid (Zyvox)
Oxazolidinone
mg
4.7
-
600 mg IV or oral every 12 hours
MAOI interaction; caution with serotonergic drugs. Effective against VRE and MRSA; Monitor for thrombocytopenia and serotonin syndrome.
Fosfomycin (Monurol)
Phosphonic Acid Derivative
mg
6.0
-
3,000 mg IV every 6 hours
Avoid in fosfomycin allergy; monitor sodium levels, avoid in hypernatremia or heart/kidney disease. Applicable for CRE, MRAB.
Lipidology
Hyperlipidemia: Classification, Diagnosis, and Management
Hyperlipidemia is a condition characterized by elevated levels of lipids in the blood, which increases the risk of cardiovascular diseases. It can be classified into primary (genetic) and secondary (acquired) types. Understanding these classifications aids in effective diagnosis and management.
Classification of Hyperlipidemia
(A) Primary Hyperlipidemia
Primary hyperlipidemia is caused by genetic defects affecting lipid metabolism. The following table summarizes the different types, their distinguishing features, and management strategies.
Secondary hyperlipidemia results from other conditions or lifestyle factors influencing lipid metabolism.
Cause
Mechanism
Management
Diabetes Mellitus
Insulin deficiency/resistance leading to increased VLDL production
Glycemic control, Statins
Hypothyroidism
Decreased LDL receptor activity
Thyroid hormone replacement
Nephrotic Syndrome
Increased hepatic lipoprotein synthesis
Treat underlying renal disease
Alcoholism
Increased VLDL synthesis
Alcohol cessation, Fibrates
Medications (e.g., beta-blockers, thiazides)
Altered lipid metabolism
Medication review and adjustment
Mechanisms of Lipid-Lowering Medications
Understanding the mechanisms helps in selecting appropriate medications based on the lipid profile and provides foundational knowledge essential for clinical examinations such as the USMLE Step 1.
Medication Class
Mechanism_of_Action
Indications
Examples and Dosages
Side Effects
Contraindications
Statins
Inhibit HMG-CoA reductase, decreasing cholesterol synthesis and upregulating LDL receptors
Gastrointestinal symptoms, increased bleeding risk at high doses
Fish allergy, bleeding disorders
Prescribing Considerations Based on Mechanism
A comprehensive understanding of the pharmacodynamics and pharmacokinetics of lipid-lowering agents is crucial for effective management.
(A) Statins
Statins are the first-line therapy for elevated LDL cholesterol due to their potent LDL-lowering effects and proven benefits in reducing cardiovascular events. They work by inhibiting the enzyme HMG-CoA reductase, a key enzyme in the cholesterol biosynthesis pathway (mevalonate pathway). This inhibition leads to decreased cholesterol synthesis in the liver and upregulation of LDL receptors on hepatocytes, enhancing the clearance of LDL from the bloodstream.
HMG-CoA Reductase (inhibited by statins)
↓
Decreased Cholesterol Synthesis in Liver
↓
Upregulation of LDL Receptors on Hepatocytes
↓
Increased Clearance of LDL from Blood
Benefits: Particularly effective in patients at high risk of cardiovascular disease, including those with familial hypercholesterolemia or existing atherosclerosis.
Monitoring: Essential to consider potential drug-drug interactions, especially with medications metabolized by the CYP3A4 enzyme system.
Side Effects: Monitor liver enzymes periodically to detect hepatotoxicity early. Be alert for signs of myopathy.
(B) Fibrates
Fibrates are the treatment of choice for patients with significant hypertriglyceridemia (Types III, IV, V) as they effectively lower triglyceride levels and can modestly increase HDL cholesterol. They activate peroxisome proliferator-activated receptor alpha (PPAR-α), which plays a role in lipid metabolism by increasing lipoprotein lipase activity and reducing VLDL production.
Activation of PPAR-α by Fibrates
↓
Lipoprotein Lipase Activity ↑ VLDL Production ↓
↓ ↓
Enhanced Breakdown of Triglycerides Less VLDL Secreted by Liver
↓ ↓
Decreased Triglyceride Levels in Blood
Benefits: Useful in preventing pancreatitis in patients with very high triglycerides.
Caution: Increased risk of myopathy when combined with statins. Assess renal function before initiating therapy.
(C) Niacin
Niacin is used when both LDL and triglycerides are elevated, and HDL cholesterol is low. It inhibits hepatic VLDL synthesis, which subsequently reduces LDL levels and increases HDL levels. This is achieved through the inhibition of diacylglycerol acyltransferase-2, leading to decreased triglyceride synthesis and VLDL formation.
Niacin Inhibits VLDL Synthesis in Liver
↓
Decreased VLDL Production
↓
Reduced LDL Levels (as LDL is a VLDL derivative)
↓
Increased HDL Levels (mechanism not fully understood)
Side Effects: Flushing (can be mitigated with aspirin), hyperglycemia, hepatotoxicity.
Contraindications: Avoid in patients with active liver disease or severe peptic ulcer disease.
(D) Bile Acid Sequestrants
These agents are suitable for patients who cannot tolerate statins or require additional LDL cholesterol reduction. They function by binding bile acids in the intestine, preventing their reabsorption. This leads to increased conversion of cholesterol into bile acids in the liver, thereby reducing hepatic cholesterol levels and upregulating LDL receptors to clear more LDL from the blood.
Bile Acid Sequestrants Bind Bile Acids in Intestine
↓
Prevents Reabsorption of Bile Acids
↓
Liver Uses Cholesterol to Synthesize More Bile Acids
↓
Decreased Hepatic Cholesterol Levels
↓
Upregulation of LDL Receptors
↓
Increased Clearance of LDL from Blood
Usage: Can be used alone or with other lipid-lowering medications.
Side Effects: May interfere with absorption of fat-soluble vitamins and other drugs.
Administration: Timing is important; other medications should be taken 1 hour before or 4 hours after.
(E) Ezetimibe
Ezetimibe provides additional LDL cholesterol reduction by inhibiting the Niemann-Pick C1-Like 1 (NPC1L1) protein involved in intestinal cholesterol absorption. This reduces the amount of cholesterol delivered to the liver, enhancing clearance of LDL from the bloodstream.
Ezetimibe Inhibits NPC1L1 Protein
↓
Reduced Cholesterol Absorption in Small Intestine
↓
Less Cholesterol Delivered to Liver
↓
Upregulation of LDL Receptors
↓
Increased Clearance of LDL from Blood
Usage: Especially useful when combined with statins for additional LDL reduction.
Monitoring: Watch for potential liver enzyme elevations when used with statins.
(F) PCSK9 Inhibitors
PCSK9 inhibitors are indicated for familial hypercholesterolemia or patients not reaching LDL cholesterol goals despite maximum tolerated statin therapy. They work by binding to proprotein convertase subtilisin/kexin type 9 (PCSK9), a protein that degrades LDL receptors on hepatocytes. By inhibiting PCSK9, these medications increase the availability of LDL receptors, enhancing LDL clearance.
PCSK9 Inhibitors Bind to PCSK9 Protein
↓
Prevent Degradation of LDL Receptors
↓
Increased LDL Receptor Availability on Hepatocytes
↓
Enhanced Clearance of LDL from Blood
Administration: Subcutaneous injections.
Considerations: High cost; reserved for specific populations. Monitor for injection site reactions.
(G) Omega-3 Fatty Acids
Used primarily in patients with severe hypertriglyceridemia to reduce the risk of pancreatitis. Omega-3 fatty acids reduce hepatic VLDL synthesis and increase triglyceride clearance by enhancing the activity of lipoprotein lipase.
Omega-3 Fatty Acids Reduce VLDL Synthesis
↓
Decreased Secretion of VLDL by Liver
↓
Enhanced Activity of Lipoprotein Lipase
↓
Increased Clearance of Triglycerides from Blood
Usage: Can be combined with other lipid-lowering therapies.
Side Effects: Be cautious of increased bleeding risk at high doses.
Contraindications: Patients with fish allergies should avoid certain formulations.
Written on October 21, 2024
Neurology
Criteria for Prescribing Dementia Medications
This document provides a detailed overview of the criteria for prescribing dementia medications in South Korea, including donepezil and other oral medications and patches. The guidelines aim to support healthcare professionals in making informed and compliant prescribing decisions, adhering to the regulatory standards set by the Health Insurance Review & Assessment Service (HIRA).
Table 1: Dementia Medications in South Korea
Generic Name
Brand Name
Form
_____________Dosage____________
_______Indications________
Contraindications
_____Side_Effects_____
Donepezil
Aricept
Oral Tablet
Starting Dose: 5 mg once daily
Maintenance Dose: 5-10 mg once daily
Mild to Moderate Alzheimer's Disease
Hypersensitivity to donepezil or piperidine derivatives
Nausea, diarrhea, insomnia, muscle cramps
Rivastigmine
Exelon
Oral Capsule
Starting Dose: 1.5 mg twice daily
Maintenance Dose: Increase by 3 mg/day every 2 weeks up to 6 mg twice daily
Mild to Moderate Alzheimer's Disease Parkinson's Disease Dementia
Hypersensitivity to rivastigmine or carbamate derivatives
Nausea, vomiting, weight loss, dizziness
Rivastigmine Patch
Exelon Patch
Transdermal Patch
Starting Dose: 4.6 mg/24h patch
Maintenance Dose: Increase to 9.5 mg/24h after 4 weeks
Maximum Dose: 13.3 mg/24h
Mild to Moderate Alzheimer's Disease Parkinson's Disease Dementia
Skin reactions at application site, hypersensitivity
Skin irritation, nausea, vomiting
Galantamine
Razadyne
Oral Tablet, Capsule
Starting Dose: 4 mg twice daily
Maintenance Dose: Increase by 8 mg/day every 4 weeks up to 12 mg twice daily
Mild to Moderate Alzheimer's Disease
Severe hepatic or renal impairment, hypersensitivity
Indicated for moderate to severe Alzheimer's disease
Coverage applicable with MMSE score of 15 or lower
Notes on Cognitive Assessment Scales:
MMSE (Mini-Mental State Examination): A score ranging from 0 to 30, with lower scores indicating more severe cognitive impairment.
CDR (Clinical Dementia Rating): Stages range from 0 (no dementia) to 3 (severe dementia).
GDS (Global Deterioration Scale): Stages range from 1 (no cognitive decline) to 7 (very severe cognitive decline).
Mechanism of Action of Dementia Medications
(A) Cholinesterase Inhibitors
Cholinesterase inhibitors, including donepezil, rivastigmine, and galantamine, function by inhibiting the enzyme acetylcholinesterase. This inhibition results in increased levels of acetylcholine in the synaptic cleft, thereby enhancing cholinergic neurotransmission. The cholinergic system is critical for cognitive processes such as memory and learning, which are typically impaired in Alzheimer's disease.
Donepezil: Selectively inhibits acetylcholinesterase, leading to prolonged action of acetylcholine in the brain.
Rivastigmine: Inhibits both acetylcholinesterase and butyrylcholinesterase, providing a broader inhibition of cholinesterase enzymes.
Galantamine: Inhibits acetylcholinesterase and modulates nicotinic receptors, which may contribute to its cognitive-enhancing effects.
(B) NMDA Receptor Antagonists
Memantine belongs to the class of NMDA (N-methyl-D-aspartate) receptor antagonists. It acts by blocking NMDA receptors, which are involved in excitatory neurotransmission and synaptic plasticity. Overactivation of NMDA receptors by glutamate can lead to excitotoxicity, contributing to neuronal damage in Alzheimer's disease. Memantine's antagonistic action helps to regulate glutamate activity, thereby protecting neurons from excitotoxicity.
(C) Combination Therapies
The combination of memantine and donepezil leverages the distinct mechanisms of action of both drugs. While donepezil enhances cholinergic neurotransmission, memantine modulates glutamatergic activity. This synergistic approach aims to address multiple pathways involved in the pathophysiology of Alzheimer's disease, potentially offering enhanced therapeutic benefits compared to monotherapy.
It is recommended to consult the latest clinical guidelines and engage in ongoing professional development to ensure the most current and effective treatment strategies are employed in dementia care.
Written on October 21, 2024
Mental Status Levels
Integrated Descriptive and Feature-Based Classification (From Most Active to Least Active)
Level of Mental Status
Description
Awareness of Self/Surroundings
Response to Verbal Stimuli
Response to Painful Stimuli
Purposeful Movement
Sleep-Wake Cycle
Any Communication
Brainstem Reflexes
Alert
Fully aware, oriented, and responsive; normal cognitive function.
O
O
O
O
O
O
O
Delirium
Disturbed attention and awareness with confusion, agitation, or hallucinations.
O (Impaired)
O (Confused)
O
O (Disorganized)
O
O (Disorganized)
O
Lethargy (Drowsy)
Reduced alertness; can be awakened easily, but responses are slow and subdued.
O (Reduced)
O (Slow)
O (Slowed)
O (Reduced)
O
O (Slower)
O
Obtundation
Significantly lowered alertness; moderate stimuli required to elicit a response.
O (Markedly Reduced)
O (Requires Effort)
O (Requires Effort)
O (Minimal)
O
O (Minimal)
O
Stupor
Profound unresponsiveness; only vigorous stimulation yields any limited response.
X (Minimal)
X (Requires Vigorous)
O (With Strong Stimuli)
X (Very Limited)
O
X (Very Limited)
O
Semi-Coma
Very deep unresponsiveness, deeper than stupor but not fully comatose.
Presence of sleep-wake cycles without awareness; reflexive actions only.
X
X
O (Reflexive Only)
X (Reflexive Only)
O
X
O
Coma
Unarousable unconsciousness; no response to any type of stimulus.
X
X
X
X
X
X
O
Brain Death
Complete and irreversible loss of all brain function and activity.
X
X
X
X
X
X
X
Suggested Communication Approach
When explaining these conditions, it is helpful to use simple, direct language and avoid overly technical terms. Highlighting what the individual can or cannot do (for example, whether they can open their eyes, respond to voices, or show any purposeful movement) allows for easier comprehension. Adopting a calm, supportive tone helps reduce anxiety and ensures that families and patients understand both the current situation and the potential implications for care and recovery.
Written on December 9th, 2024
Restless syndrome: Causes and coping methods (Written March 7, 2025)
Restless syndrome—often associated with restless legs syndrome—is a condition that leads to an uncontrollable urge to move certain parts of the body, typically the legs. This restlessness, which often intensifies during periods of inactivity or rest, can significantly disrupt daily life. A comprehensive review of causes, symptoms, and management strategies is provided below.
Underlying Cause
Characteristics
Recommended Interventions
Iron deficiency
Lower-than-normal iron levels affecting dopamine function
Iron supplementation and iron-rich diet
Chronic diseases
Diabetes, kidney disease, autoimmune disorders
Condition-specific management and medication
Medication-induced
Certain antihistamines, antidepressants, and antipsychotics
Adjusting doses or changing prescriptions
Peripheral neuropathy
Nerve damage leading to heightened sensations
Neuropathic pain management, physical therapy
Lifestyle factors
Excess caffeine, alcohol, smoking, high stress
Reduced substance intake, relaxation techniques
I. Overview
Definition
Restless syndrome is characterized by an uncomfortable or tingling sensation in the limbs, leading to an irresistible need for movement. Although the legs are most commonly affected, other parts of the body may also experience similar symptoms.
Prevalence and significance
Common in various age groups, with a higher incidence in middle-aged to older adults.
Can interrupt sleep, reduce daytime productivity, and adversely impact overall quality of life.
II. Causes
Neurological factors
Imbalance in dopamine levels within the central nervous system is frequently associated with restless syndrome. Proper neurotransmitter regulation is crucial for smooth muscle control and movement coordination.
Genetic predisposition
A family history of restless syndrome has been observed in numerous cases, suggesting a genetic component. Early onset is especially correlated with inherited factors.
Underlying medical conditions
Iron deficiency: Low iron levels in the brain can contribute to abnormal dopamine function.
Chronic diseases: Kidney disease, diabetes, and certain autoimmune disorders have been linked to symptoms of restlessness.
Peripheral neuropathy: Damage to peripheral nerves may amplify sensations that trigger restlessness.
Lifestyle and external influences
Medication side effects: Some antihistamines, antidepressants, and antipsychotics may exacerbate restlessness.
Substance intake: Excessive caffeine, alcohol, and nicotine use can heighten symptoms.
Stress and anxiety: Emotional distress and prolonged psychological tension often intensify discomfort and restlessness.
III. Key symptoms
Uncomfortable sensations
Tingling, itching, or crawling feelings in the lower limbs.
Urges for movement generally worsen during extended periods of inactivity.
Sleep disruption
Onset or worsening of symptoms during the night.
Frequent awakenings and non-restorative sleep lead to daytime fatigue.
Relief upon movement
Temporary symptom alleviation is often experienced when walking, stretching, or shaking the affected area.
IV. Management strategies
Lifestyle modifications
Healthy sleep habits: Adherence to consistent bedtimes and a relaxing nighttime routine can mitigate sleep disturbances.
Moderation of stimulants: Limiting caffeine, alcohol, and tobacco consumption lowers aggravating factors.
Physical activity: Mild to moderate exercise, such as stretching or low-impact aerobics, may alleviate symptoms. Overly intense workouts, however, are best approached with caution.
Nutritional support
Balanced diet: Adequate intake of iron, folate, and magnesium is strongly recommended.
Dietary supplements: Professional consultation may determine the need for iron supplementation or vitamins.
Medical interventions
Pharmacological therapy: Dopamine agonists and certain anti-seizure medications are frequently prescribed.
Addressing underlying conditions: Correcting iron deficiency or managing chronic diseases helps reduce restlessness.
Medication adjustments: Healthcare professionals may recommend altering existing prescriptions that intensify symptoms.
Stress reduction techniques
Mindfulness and relaxation: Breathing exercises, meditation, or yoga may lessen psychological triggers.
Professional counseling: Therapy sessions help identify stress factors contributing to restlessness.
Written on March 7, 2025
Pharmacological Management of Sleep Disturbances and Delirium in Elderly Patients in LTCFs (Written March 26, 2025)
Elderly patients in long-term care facilities (LTCFs) commonly experience sleep disturbances or delirium. While non-pharmacological measures—such as optimizing the sleep environment, maintaining consistent sleep–wake schedules, and reducing nighttime noise—are always the first line, pharmacological therapy may be needed when these measures prove inadequate.
Due to altered metabolism, higher sensitivity, and polypharmacy concerns in older adults, clinicians must prescribe sedatives, hypnotics, and antipsychotics judiciously. The guiding principle is to use the lowest effective dose for the shortest duration, with frequent reassessment to minimize risks such as falls, respiratory depression, excessive sedation, and worsening confusion.
Classification of Medications (Mild to Severe)
Below is a general framework for medications used for insomnia or delirium in older adults, arranged roughly from those with milder effects and fewer side effects to agents reserved for more severe agitation or psychotic symptoms:
2–5 mg daily (initiate at 2 mg and titrate slowly)
Delirium with psychotic features; alternative when sedation risk is high
– Dementia-related psychosis caution
– Parkinson’s disease (may still pose EPS risk)
– History of NMS
– Akathisia (restlessness)
– Possible EPS
– Insomnia or sedation (varies)
– Metabolic changes
Haloperidol (PO/IM/IV)
PO: 0.5–2 mg daily in divided doses (mild delirium/agitation); up to 5 mg in severe cases IM/IV: 0.5–2 mg for acute severe agitation (may repeat carefully as needed)
Severe delirium, psychosis, or agitation unresponsive to other measures
– Parkinson’s disease
– Lewy body dementia
– High risk of EPS & tardive dyskinesia
The table below provides a stepped approach based on symptom severity (mild insomnia to severe agitation/psychosis), with corresponding dosage ranges. Always start low and titrate slowly in elderly patients.
Medication
Mild Presentation
Moderate Presentation
Severe Presentation
Melatonin
2 mg at bedtime
–
–
Low-dose Doxepin
3 mg at bedtime
6 mg at bedtime
–
Trazodone
25 mg at bedtime
50–75 mg at bedtime
100 mg at bedtime (rarely needed for insomnia alone)
Mirtazapine
7.5 mg at bedtime
15 mg at bedtime
15 mg or higher (caution: sedation, weight gain)
Zolpidem
5 mg at bedtime
10 mg at bedtime (short term)
– (Generally not indicated for severe delirium/agitation)
Alprazolam
0.25 mg once or twice daily PRN
0.5 mg TID (short term for anxiety/agitation)
– (Usually not first-line for severe agitation/delirium)
Lorazepam (PO)
0.5 mg at bedtime or PRN
1–2 mg/day in divided doses
–
Lorazepam (IV)
–
0.5–1 mg IV for acute agitation
2 mg IV (extreme agitation; close monitoring)
Quetiapine
12.5 mg at bedtime (mild insomnia/mild delirium)
25–50 mg at bedtime or split doses (moderate agitation/psychosis)
100 mg or higher (severe agitation; titrate cautiously)
Risperidone
0.25 mg daily
0.5–1 mg daily
2 mg daily (severe agitation/psychosis; monitor for EPS)
Aripiprazole
2 mg daily (initiate low)
2–5 mg daily (titration based on response)
5 mg or higher (severe agitation/psychosis; monitor for akathisia, EPS)
Haloperidol (PO)
0.5 mg in divided doses (mild delirium)
Up to 2 mg/day in divided doses (moderate agitation/psychosis)
5 mg/day (severe cases; increased EPS risk)
Haloperidol (IM/IV)
–
0.5–1 mg for acute agitation (may repeat carefully)
2–5 mg for severe acute agitation; watch for QT prolongation, EPS
Written on March 26, 2025
Management of nocturnal “cat-like” vocalizations in a psychiatric inpatient (Written May 22, 2025)
🔍 Background and clinical concern
Nocturnal animal-like sounds may disturb ward milieu and sleep quality of fellow inpatients.
Respectfully identifying the underlying mechanism precedes pharmacological changes, in order to avoid unnecessary dose escalation and to tailor supportive measures.
🧩 Differential considerations
1. Catathrenia (sleep-related expiratory groan)
Prolonged, monotonic expiratory sound during rapid-eye-movement or non-REM sleep.
Patient typically unaware; no daytime psychiatric or neurologic sequelae.
Confirmation: full-night polysomnography (PSG) with audio–video channel.
2. Residual psychotic or mood symptoms
Animal-like vocalization may accompany hallucination, delusional content, or affective excitation.
Evaluate for other positive or affective features; review Mental Status Examination notes.
3. Drug-induced motor phenomena
Aripiprazole can rarely provoke tic-like utterances or tardive dyskinesia manifesting as brief cries.
Temporal relationship to recent dose change strengthens suspicion.
4. Obstructive sleep apnoea (OSA) and weight-related airway narrowing
Quetiapine may worsen OSA via weight gain and myorelaxant action.
Consider simultaneously during PSG study.
🪜 Recommended stepwise approach
Step
Action
Key notes
1
Obtain 1–3 nights of bedside audio–video monitoring
Document timing, duration, and coupling with respiratory cycle.
2
Arrange PSG ± titration CPAP trial
Rule out catathrenia and co-existing OSA.
3-A
Confirmed catathrenia
Initiate auto-CPAP or fixed CPAP.
If partial response, consider bedtime clonazepam 0.25–1 mg (monitor falls).
3-B
Psychiatric symptom persistence
Gradual increase aripiprazole → 15–20 mg or switch to risperidone/olanzapine.
For tic or tardive phenomena, reduce aripiprazole ≤ 5 mg; add propranolol 20–40 mg.
4
Optimise hypnotic regimen
Administer quetiapine 100 mg as single dose 30 min before sleep.
Titrate within 50–300 mg based on sedation and metabolic profile.
5
Environmental modifications
Offer private room if feasible; provide earplugs or white-noise device to cotenants.
At bedtime
• Quetiapine 100 mg PO once daily
• Clonazepam 0.5 mg PO once daily PRN (maximum 7 nights)
Daytime
• Aripiprazole 10 mg PO once daily
Evaluate response after 7 days; taper clonazepam if satisfactory.
Introduce CPAP immediately if PSG confirms catathrenia.
⚠️ Monitoring and safety
Falls & over-sedation: check orthostatics and gait twice daily during first week of clonazepam.
Metabolic parameters: weight, fasting glucose, lipid panel weekly while quetiapine is titrated.
Extrapyramidal status: monthly AIMS screening for tardive dyskinesia.
📑 Summary
Prioritising careful differential diagnosis safeguards the patient from unwarranted antipsychotic escalation and preserves ward harmony.
Stepwise assessment—objective sleep recording, polysomnography, judicious pharmacological adjustment, and environmental support—addresses the complaint with minimal iatrogenic risk.
Continuous monitoring of cardiometabolic and neuromotor parameters remains essential throughout therapy optimisation. 🙏
Written on May 22, 2025
Night-time sedation assessment for acting-out patient (Written June 24, 2025)
The following review humbly integrates dosing-time information (HS, at bedtime; QE, every evening) into the previous analysis, lists the Korean brand names of behaviour-modifying agents, and evaluates proposed additional sedatives for their capacity to induce night-time sleep.:contentReference[oaicite:0]{index=0}
Risperidone 3 mg HS balances hypnotic depth with behavioural control; however, cerebrovascular and metabolic risks necessitate diligent monitoring.
Lorazepam 2 mg IM HS provides the most rapid and profound sedation but carries the greatest risk of respiratory depression and delirium; reserve for severe, unmanageable agitation after other measures fail.
Lorazepam 1 mg PO BID is suitable for anticipatory anxiety but may lose efficacy as tolerance develops; avoid long-term reliance.
Haloperidol 2.25 mg HS offers antipsychotic control yet produces lighter sleep and higher extrapyramidal liability compared with atypical antipsychotics or benzodiazepines.
Recommendations
Optimise existing evening quetiapine and risperidone before introducing additional high-potency sedatives.
When rapid tranquillisation is essential, prefer single-agent lorazepam IM with continuous monitoring, limiting course to the briefest necessary period.
Combine pharmacologic strategies with non-drug interventions (environmental cues, daytime activity) to consolidate nocturnal sleep.
Written on June 24, 2025
Seizure Medications (Written March 28, 2025)
1. Sodium Channel Blockers
Medication
Brand Names
Typical Adult Dosing
Indications (Ix)
Contraindications (CIx)
Common Side Effects
Description
Lamotrigine
Lamictal
- Start 25 mg/day, titrate slowly to 100–200 mg/day
- Up to 400 mg/day in severe cases (slow titration crucial)
Focal and generalized seizures; also used in bipolar disorder
Known hypersensitivity; caution when used with valproate (requires slower titration)
- Loading: 5–15 mg/kg IV
- Maintenance: 0.5–5 mg/kg/hr infusion
Refractory status epilepticus requiring barbiturate coma
Porphyria, severe respiratory depression
Profound sedation, hypotension, respiratory depression, decreased GI motility, ileus
Used if other IV sedatives fail; continuous EEG monitoring essential
Thiopental
Pentothal (older)
- Similar to pentobarbital (variable infusion rates to achieve burst suppression)
Refractory status epilepticus requiring barbiturate coma
Porphyria, severe respiratory depression
Hypotension, respiratory depression, potential for arrhythmias, myocardial depression
Barbiturate with rapid onset; requires close BP and cardiac monitoring
5. Recommendations by Clinical Scenario
Below is a quick‐reference guide that organizes treatments by severity. Dosing ranges are included for immediate bedside reference, though exact regimens may vary depending on patient weight, comorbidities, and institutional protocols.
★ Mild to Moderate Seizures
Initiate Oral Monotherapy
Levetiracetam (Keppra, Keppra XR): 500–1,000 mg twice daily; may go up to 1,500 mg twice daily
Valproate (Depakote): 10–30 mg/kg/day in divided doses
Lamotrigine (Lamictal): 25 mg/day initially, titrate to 100–200 mg/day
Carbamazepine (Tegretol): 200 mg twice daily, titrate to 800–1,200 mg/day
Topiramate (Topamax): 25–50 mg/day initially, titrate to 200–400 mg/day
Adjunctive or Add-On Therapy
Gabapentin (Neurontin): 900–1,800 mg/day in divided doses
Pregabalin (Lyrica): 150–600 mg/day in divided doses
Clonazepam (Klonopin): 0.5–2 mg/day in divided doses if intermittent benzodiazepine needed
★ Moderate to Severe Seizures
Oral or Initial Intravenous Therapy
Valproate (Depakote IV): Loading 20–40 mg/kg, then 15–60 mg/kg/day
Lorazepam (Ativan): 0.1 mg/kg IV (max 4 mg/dose); may repeat once
Diazepam (Valium): 5–10 mg IV, may repeat; or 0.15 mg/kg in status settings
★ Status Epilepticus
First‐Line: Benzodiazepines
Lorazepam (Ativan): 0.1 mg/kg IV (max 4 mg/dose), may repeat once
If no IV access: Midazolam (Versed): 0.2 mg/kg IM (or intranasal/buccal), or Diazepam (Valium): 0.15 mg/kg rectal
Second‐Line (After Benzodiazepines)
Fosphenytoin/Phenytoin (Dilantin): Loading 15–20 mg PE/kg IV
Valproate (Depakote IV): Loading 20–40 mg/kg
Levetiracetam (Keppra IV): Loading 2–4 g
Refractory Status Epilepticus
Continuous infusions to achieve burst suppression (guided by continuous EEG):
Midazolam (Versed) Infusion
Propofol (Diprivan) Infusion
Pentobarbital/Thiopental
Ketamine infusion (1–2 mg/kg/hr) can be considered in super‐refractory cases
Written on March 28, 2025
Management of hiccups with pharmacotherapy (Written May 19, 2025)
딸꾹질(hiccup, singultus)은 횡격막이 불수의적으로 수축하면서 성대가 급격히 닫혀 발생하는 특징적 “hic” 음을 동반하는 현상이다. 48 시간 이상 지속되면
persistent
, 1 개월 이상이면
intractable
로 정의하며, 이 단계에서는 수면·섭식 장애, 흉복부 통증, 탈수·전해질 이상 등이 동반될 수 있어 약물치료가 권고된다.
근본 질환 교정이 최우선이나, 원인이 불명확하거나 교정 불가능할 때는 증상 완화를 위해 약물 요법을 시행한다. 약물 선택은 근거 수준·환자 기저질환·부작용 프로파일을 모두 고려하여 단계적으로 진행한다.
1차 선택 약물
💊 Baclofen (바클란 정)
용량·용법
– 5 – 10 mg 경구 1일 3회로 시작, 48–72 시간 간격으로 5 – 10 mg씩 증량하여 40 – 80 mg/일 범위 유지
치료 원칙
– 중추성 원인(뇌졸중‧외상 등)에 특히 효과적이며, 신부전 시 감량 필요
주의
– 갑작스러운 중단은 금기, 졸림·어지럼증·저혈압 모니터링
대안·병용 가능 약제 한눈에 보기
💊 약제
용량·용법
Ix
CIx
주요 부작용
설명
Chlorpromazine
25 – 50 mg PO/IV/IM q6–8 h (≤ 200 mg/일)
FDA 승인 난치성 딸꾹질
CNS 억제, 중증 심혈관‧골수 억제
기립성 저혈압, 진정, 추체외로 증상
D
2
차단·진정 작용으로 횡격막 반사 억제
Metoclopramide
10 mg PO/IV q8 h (≤ 40 mg/일)
말초성(위식도 관련) 딸꾹질
장폐색, 위장관 출혈, 파킨슨병
졸림, 불안, EPS
D
2
/5-HT
3
길항·위배출 촉진
Gabapentin
100 – 300 mg HS 시작 → 300 mg TID, 목표 0.9 – 2.4 g/일
중추병변·신부전 등 바클로펜 제한 시
중증 신부전(감량), 과민 반응
현훈, 체중 증가, 부종, 진정
Ca
2+
채널 α
2
δ 서브유닛 결합, 신경 흥분 억제
Haloperidol
2 – 5 mg PO/IM q8–12 h (≤ 20 mg/일)
정신증 동반·다른 약제 실패 시
QT 연장, 파킨슨병, 중증 CNS 억제
EPS, QT 연장, 진정
D
2
강력 차단으로 중추 흥분 억제
Pregabalin
75 mg BID 시작 → 300 – 450 mg/일 목표
Gabapentin 불내성/효과 부족 시
중증 심‧신부전, 과민 반응
부종, 체중 증가, 진정, 어지럼
Ca
2+
채널 α
2
δ 결합, 신경 흥분 억제
Valproic acid
250 mg TID → 15 mg/kg/일
간질·편두통 동반 환자
활동성 간질환, 임신 1분기
간독성, 췌장염, 체중 증가
GABA 농도↑; 증례 보고 기반
Nifedipine
10 mg PO TID PRN
고혈압·협심증 동반
중증 저혈압, 심부전
말초 부종, 두통, 안면 홍조
L-형 Ca
2+
차단으로 횡격막 수축 억제 추정
투여 순서·병용 전략
원인 검색
– 구조적·대사성·약물성 요인 교정이 최우선.
Baclofen 5–10 mg TID
로 시작, 필요 시 증량(신부전 감량).
불응 시
chlorpromazine, gabapentin, metoclopramide 중 환자 상태에 맞춰 추가·교체.
지속되면 haloperidol·pregabalin 등 2차 약제 고려, QT·신기능 모니터링.
약물치료 실패 시 phrenic/vagal block, 전기자극 등 시술적 방법 검토.
임상 적용 시 유의 사항
용량-반응
곡선 차이를 고려하여 증량 단계마다 48–72 시간 이상 관찰.
EPS 등
신경계 부작용
발생 시 속효성 항콜린제(예: diphenhydramine)로 대응.
고령·다질환
환자는 기립성 저혈압·혼동 위험이 높으므로 “start low, go slow” 원칙 적용.
본 자료는 최신 문헌·FDA 라벨을 기반으로 한 전문가 참고용이며, 실제 처방은 환자 특성·임상 판단에 따라야 한다.
Written on May 19, 2025
Endocrinology
Diabetes Medications (Written December 15, 2024)
Medication Class
Product Name
Mechanism of Action
Dosage (Typical)
Indications
Contraindications
Side Effects
Additional Details
Biguanides
Metformin (Glucophage, Glucophage XR, others)
Inhibits hepatic gluconeogenesis by activating AMP-activated protein kinase (AMPK).
Enhances peripheral insulin sensitivity.
Increases glucose uptake in skeletal muscle.
500 mg twice daily to 2000 mg/day (divided doses)
First-line therapy for Type 2 Diabetes Mellitus.
Favored in patients with overweight or obesity.
Suitable for patients with cardiovascular risk factors.
Renal impairment: eGFR < 30 mL/min/1.73 m².
Significant hepatic disease.
Acute conditions predisposing to lactic acidosis.
Common:
Nausea
Diarrhea
Abdominal discomfort
Serious:
Lactic acidosis
Vitamin B12 deficiency
Renal Considerations: Not indicated in patients with reduced renal function.
Weight neutrality or modest weight loss.
Requires monitoring of renal function and vitamin B12 levels periodically.
Should be taken with meals to reduce gastrointestinal side effects.
Contraindicated in patients with significant hepatic disease or acute conditions predisposing to lactic acidosis.
Sulfonylureas
Glipizide (Glucotrol)
Stimulates insulin secretion from pancreatic β-cells.
Binds to SUR1 subunit of K_ATP channels, causing cell membrane depolarization and insulin release.
5 mg once daily to 40 mg/day (depending on formulation)
Preferred for patients needing potent insulin secretagogues.
Beneficial when rapid onset is required.
Suitable for patients who can adhere to meal schedules.
Renal impairment: Increased risk of hypoglycemia.
Hypersensitivity to sulfonylureas.
Common:
Hypoglycemia
Weight gain
Less Common:
Dermatologic reactions
Gastrointestinal disturbances
Renal Considerations: Caution in patients with renal impairment.
Requires meals to prevent hypoglycemia.
Not recommended in patients with significant hepatic or renal impairment.
May require dose adjustment in elderly patients.
Regular monitoring of blood glucose levels is essential to minimize the risk of hypoglycemia.
Glyburide (Diabeta, others)
Stimulates insulin secretion from pancreatic β-cells.
Binds to SUR1 subunit of K_ATP channels, leading to insulin release.
1.25 mg to 20 mg/day (depending on formulation)
Suitable for patients requiring long-acting insulin secretagogues.
Beneficial in patients at higher risk of nocturnal hypoglycemia.
Renal impairment: Increased risk of prolonged hypoglycemia.
Cardiovascular disease (with caution).
Common:
Hypoglycemia
Weight gain
Less Common:
Cardiovascular events
Dermatologic reactions
Renal Considerations: Increased risk of prolonged hypoglycemia in renal impairment.
Higher risk of hypoglycemia compared to other sulfonylureas, especially in elderly patients.
Should be used with caution in patients with renal or hepatic impairment.
Regular monitoring of blood glucose is necessary to adjust doses appropriately.
Glimepiride (Amaryl)
Binds to SUR1 receptor on pancreatic β-cells.
Causes closure of K_ATP channels, leading to membrane depolarization and insulin secretion.
Longer duration with lower hypoglycemia risk.
1 mg to 8 mg/day
Preferred for patients needing effective glycemic control with lower hypoglycemia risk.
Beneficial for patients with irregular meal schedules due to longer action.
Renal impairment: Increased risk of hypoglycemia.
Hepatic impairment: Use with caution.
Hypersensitivity to sulfonylureas.
Common:
Hypoglycemia (less frequent)
Weight gain
Less Common:
Gastrointestinal disturbances
Allergic reactions
Renal Considerations: Use with caution in renal impairment due to increased hypoglycemia risk.
More favorable side effect profile regarding hypoglycemia compared to other sulfonylureas.
May be preferred in patients at risk of hypoglycemia or requiring once-daily dosing.
Regular blood glucose monitoring is essential to ensure efficacy and safety.
Meglitinides
Repaglinide (Prandin)
Binds to SUR1 subunit of pancreatic β-cell K_ATP channels.
Causes rapid, short-term closure leading to insulin secretion.
Faster onset and shorter duration compared to sulfonylureas.
0.5 mg before meals, up to three times daily
Ideal for patients with irregular meal times.
Suitable for those requiring flexible dosing schedules.
Appropriate for combination with metformin or other non-insulin agents.
Hypersensitivity to meglitinides.
Severe hepatic impairment.
Common:
Hypoglycemia (less severe than sulfonylureas)
Weight gain
Less Common:
Gastrointestinal disturbances
Dizziness
Headache
Renal Considerations: Dose adjustment may be necessary in renal impairment to prevent hypoglycemia.
Requires precise meal timing to maximize efficacy and minimize hypoglycemia risk.
May be taken up to three times daily with meals.
Suitable for patients who experience significant postprandial hyperglycemia.
Regular monitoring of blood glucose levels is recommended.
Nateglinide (Starlix)
Stimulates rapid, short-term insulin release by binding to SUR1 subunit of K_ATP channels on pancreatic β-cells.
Leads to insulin secretion.
60 mg before meals, up to three times daily
Beneficial for patients needing control over postprandial glucose spikes.
Suitable for those requiring flexibility in meal timing.
Appropriate for combination therapy with other oral agents.
Severe hepatic impairment.
Hypersensitivity to meglitinides.
Pregnancy and breastfeeding.
Common:
Hypoglycemia (rare)
Weight gain
Less Common:
Headache
Dizziness
Gastrointestinal issues
Renal Considerations: Dose adjustment may be required in renal impairment to reduce hypoglycemia risk.
Offers flexibility in dosing with respect to meal timing.
Rapid onset and short duration may reduce hypoglycemia risk.
Requires patient education on meal planning to optimize therapeutic outcomes.
Regular monitoring is advised to ensure optimal glycemic control.
Alpha-Glucosidase Inhibitors
Acarbose (Precose)
Inhibits intestinal α-glucosidases, delaying the breakdown and absorption of complex carbohydrates in the small intestine.
Reduces postprandial hyperglycemia.
25 mg three times daily with the first bite of each main meal
Preferred for patients with postprandial hyperglycemia.
Suitable for those who can adhere to dietary modifications.
Appropriate for combination with other oral agents.
Inflammatory bowel disease.
Chronic intestinal disease with structural changes.
Inflammatory bowel disease.
Common:
Flatulence
Diarrhea
Abdominal pain
Less Common:
Bloating
Indigestion
Renal Considerations: Generally well-tolerated, but caution may be needed in patients with renal impairment.
Efficacy enhanced with strict adherence to a carbohydrate-controlled diet.
May require gradual dose titration to minimize gastrointestinal side effects.
Regular monitoring of digestive tolerance is necessary.
Miglitol (Glyset)
Inhibits intestinal α-glucosidases, slowing carbohydrate digestion and absorption.
Reduces postprandial blood glucose levels.
25 mg three times daily with the first bite of each main meal
Suitable for managing postprandial hyperglycemia in Type 2 Diabetes Mellitus.
Preferred for patients who can manage dietary carbohydrate control.
Severe hepatic impairment.
Chronic intestinal disease with structural changes.
Hypersensitivity to miglitol.
Common:
Flatulence
Diarrhea
Abdominal pain
Less Common:
Nausea
Dizziness
Renal Considerations: Dose adjustment recommended in renal impairment to prevent accumulation and exacerbated side effects.
Shorter duration of action compared to acarbose, offering some flexibility in dosing schedules.
Requires patient education on dietary carbohydrate management to optimize therapeutic outcomes.
Monitoring of gastrointestinal tolerance is essential.
Thiazolidinediones
Pioglitazone (Actos)
Acts as a PPAR-γ agonist, enhancing insulin sensitivity in adipose tissue, skeletal muscle, and liver.
Modulates gene expression related to glucose and lipid metabolism.
15-45 mg/day
Preferred for patients with insulin resistance.
Suitable for those with non-alcoholic steatohepatitis (NASH).
Beneficial for patients at risk for cardiovascular events.
Appropriate for combination with other oral agents.
Active heart failure.
History of bladder cancer (with pioglitazone).
Severe hepatic impairment.
Common:
Weight gain
Edema
Increased risk of bone fractures
Serious:
Heart failure exacerbation
Bladder cancer risk (controversial)
Renal Considerations: May cause fluid retention, contraindicated in patients with active heart failure.
Improves lipid profiles by lowering triglycerides and increasing HDL cholesterol.
Requires monitoring for signs of heart failure and regular screening for bladder cancer in long-term use.
Not recommended for patients with NYHA Class III or IV heart failure.
Rosiglitazone (Avandia)
Acts as a PPAR-γ agonist, increasing insulin sensitivity in peripheral tissues.
Enhances glucose uptake and reduces insulin resistance.
4-8 mg/day
Utilized for patients requiring significant improvement in insulin sensitivity.
Preferred for those who have not achieved glycemic control with other agents.
Suitable for combination therapy with other oral agents.
Renal Considerations: May induce fluid retention, contraindicated in heart failure patients.
Associated with increased cardiovascular risks, leading to restricted use in some regions.
Requires careful patient selection and monitoring for signs of heart failure and other adverse effects.
Regular liver function tests may be necessary.
DPP-IV Inhibitors
Sitagliptin (Januvia)
Inhibits dipeptidyl peptidase-4 (DPP-IV) enzyme.
Prevents degradation of incretin hormones (GLP-1 and GIP).
Prolongs incretin action to increase insulin secretion and decrease glucagon release in a glucose-dependent manner.
100 mg once daily
Preferred for patients seeking weight-neutral therapy.
Suitable for those with a low risk of hypoglycemia.
Appropriate for combination with most other oral agents, including metformin and SGLT-2 inhibitors.
History of pancreatitis.
Severe hepatic impairment.
Hypersensitivity to DPP-IV inhibitors.
Common:
Nasopharyngitis
Headache
Upper respiratory tract infections
Serious:
Pancreatitis (rare)
Joint pain
Hypersensitivity reactions
Renal Considerations: Dose adjustment required in severe renal impairment for some agents.
Generally weight-neutral with a low risk of hypoglycemia.
Suitable for elderly patients and those with a history of hypoglycemic episodes.
Monitoring for signs of pancreatitis and joint pain is recommended.
Saxagliptin (Onglyza)
Inhibits DPP-IV, increasing incretin levels.
Enhances insulin secretion and suppresses glucagon secretion in a glucose-dependent manner.
5 mg once daily
Suitable for patients requiring effective glycemic control without weight gain.
Preferred for those combining with other oral antidiabetic agents.
Appropriate for patients seeking low hypoglycemia risk therapies.
History of pancreatitis.
Severe hepatic impairment.
Hypersensitivity to DPP-IV inhibitors.
Common:
Upper respiratory infections
Headache
Nasopharyngitis
Serious:
Pancreatitis (rare)
Acute renal failure
Hypersensitivity reactions
Renal Considerations: Dose adjustment necessary in moderate to severe renal impairment.
May slightly increase risk for heart failure hospitalization.
Patients should be monitored for signs of heart failure, especially those with existing cardiovascular conditions.
Regular renal function tests are advised.
Linagliptin (Tradjenta)
Inhibits DPP-IV enzyme.
Elevates incretin levels, enhancing insulin secretion and reducing glucagon release in a glucose-dependent manner.
5 mg once daily
Ideal for patients with renal impairment.
Does not require dose adjustment in renal impairment.
Suitable for combination therapy with other oral antidiabetic agents.
History of pancreatitis.
Severe hepatic impairment.
Hypersensitivity to DPP-IV inhibitors.
Common:
Nasopharyngitis
Headache
Diarrhea
Serious:
Pancreatitis (rare)
Hypersensitivity reactions
Joint pain
Renal Considerations: No dose adjustment needed for renal impairment.
Convenient for patients with chronic kidney disease due to no dose adjustment requirement.
Reduces complexity of therapy in patients with renal issues.
Regular monitoring for pancreatitis and hypersensitivity is recommended.
SGLT-2 Inhibitors
Dapagliflozin (Farxiga)
Inhibits sodium-glucose co-transporter 2 (SGLT-2) in the proximal renal tubules.
Reduces glucose reabsorption and increases urinary glucose excretion.
Lowers blood glucose and promotes weight loss and diuresis.
10-20 mg once daily
Favored for patients with Type 2 Diabetes Mellitus.
Suitable for those with cardiovascular disease, heart failure, or chronic kidney disease.
Preferred for patients needing benefits beyond glycemic control.
Severe renal impairment.
History of Fournier’s gangrene.
Active bladder cancer.
Common:
Genital infections
Urinary tract infections
Increased urination
Dehydration
Serious:
Euglycemic diabetic ketoacidosis
Acute kidney injury
Fournier’s gangrene (rare)
Renal Considerations: Requires adequate renal function; less effective in severe renal impairment.
May confer cardiovascular and renal protective effects.
Monitoring for urinary and genital infections is essential.
Patients should maintain adequate hydration to prevent dehydration and renal complications.
Requires monitoring of renal function and electrolyte balance.
Ipragliflozin (specific regional name)
Inhibits SGLT-2 in the kidneys.
Enhances urinary glucose excretion, contributing to lower blood glucose levels.
Promotes weight loss and blood pressure reduction.
50 mg once daily (varies by region)
Indicated for Type 2 Diabetes Mellitus patients requiring additional glycemic control.
Favored for those benefiting from weight loss and blood pressure reduction.
Suitable for combination with other oral agents.
Severe renal impairment.
History of Fournier’s gangrene.
Active bladder cancer.
Common:
Genital mycotic infections
Urinary tract infections
Increased urination
Dehydration
Serious:
Euglycemic ketoacidosis
Acute kidney injury
Necrotizing fasciitis of the perineum (Fournier’s gangrene)
Renal Considerations: Efficacy reduced in severe renal impairment; caution needed to avoid volume depletion.
Offers cardiovascular and renal benefits similar to other SGLT-2 inhibitors.
Educate patients on maintaining personal hygiene to reduce infection risk.
Advised to stay hydrated to prevent dehydration and renal complications.
Regular monitoring of renal function and electrolyte balance is recommended.
Empagliflozin (Jardiance)
Inhibits SGLT-2 in the renal proximal tubule.
Decreases glucose reabsorption and increases urinary glucose excretion.
Lowers plasma glucose and induces osmotic diuresis, promoting weight loss and lowering blood pressure.
10-25 mg once daily
Preferred for patients with Type 2 Diabetes Mellitus.
Suitable for those with established cardiovascular disease, heart failure, or chronic kidney disease.
Favored due to proven cardiovascular and renal benefits.
Severe renal impairment.
History of Fournier’s gangrene.
Active bladder cancer.
Common:
Genital infections
Urinary tract infections
Increased urination
Dehydration
Serious:
Euglycemic diabetic ketoacidosis
Acute kidney injury
Fournier’s gangrene (rare)
Renal Considerations: Not recommended in patients with severe renal impairment; efficacy depends on adequate renal function.
Demonstrated significant reductions in cardiovascular mortality and hospitalization for heart failure.
Patients should be monitored for signs of dehydration, renal function, and potential urinary or genital infections.
Education on recognizing symptoms of ketoacidosis is essential despite its euglycemic nature.
Written on December 15th, 2024
Systematic Review of Cushing’s Syndrome and Cushing’s Disease (Written December 22, 2024)
Cushing’s syndrome is a clinical condition arising from prolonged exposure to excessive glucocorticoids. When the etiology lies in an adrenocorticotropic hormone (ACTH)-secreting pituitary adenoma, the condition is designated as Cushing’s disease. Although both terms are closely intertwined, Cushing’s disease represents a subset of Cushing’s syndrome, accounting for the majority of endogenous ACTH-dependent cases. A thorough understanding of the pathophysiology, differential diagnoses, clinical manifestations, and management strategies is fundamental for all physicians and healthcare professionals involved in patient care.
Differential Diagnosis and Classification
Cushing’s syndrome is broadly categorized based on the origin of hypercortisolism: primary (adrenal), secondary (pituitary), tertiary (hypothalamic), or exogenous (iatrogenic). The following sections provide a structured approach to differentiating these etiologies.
Prevalence of Hypertension: Reported in approximately 75–80% of patients with Cushing’s syndrome.
Osteoporosis Risk: Up to 50–60% of patients may experience reduced bone mineral density, with a significant risk of fractures.
Diabetes or Glucose Intolerance: Observed in roughly 40–50% of patients.
Diagnostic Approach
Screening Tests for Hypercortisolism
Overnight 1 mg Dexamethasone Suppression Test
Administer 1 mg dexamethasone orally at 11 PM, measure serum cortisol at 8 AM.
A cortisol level >1.8 µg/dL (50 nmol/L) is suggestive of Cushing’s syndrome in most modern assays.
24-Hour Urinary Free Cortisol (UFC)
Measures unbound cortisol excreted in the urine over 24 hours.
A value >3 times the upper limit of normal strongly indicates hypercortisolism (generally requires at least two elevated measurements).
Late-Night Salivary Cortisol
Utilizes the loss of normal diurnal variation in cortisol.
An elevated late-night salivary cortisol (typically >0.25 µg/dL or 6 nmol/L, depending on assay) can be highly sensitive for Cushing’s syndrome.
Differentiating Etiologies
Plasma ACTH Level
Low ACTH → Primary adrenal cause or exogenous steroid use.
High / Inappropriately Normal ACTH → ACTH-dependent (pituitary or ectopic).
High-Dose Dexamethasone Suppression Test (HDDST)
Helps distinguish pituitary (Cushing’s disease) from ectopic ACTH sources.
In Cushing’s disease, cortisol typically suppresses by ≥50% from baseline; ectopic ACTH-producing tumors generally do not suppress.
CRH Stimulation Test
Pituitary adenomas often show an increase in ACTH and cortisol after CRH administration.
Ectopic sources usually lack this response.
Imaging
Pituitary MRI: High-resolution MRI with gadolinium is recommended for suspected Cushing’s disease.
Adrenal Imaging (CT/MRI): Performed in cases of ACTH-independent Cushing’s or to investigate adrenal incidentalomas.
Chest/Abdominal Imaging: Required if ectopic ACTH or CRH production is suspected (e.g., small cell lung carcinoma, neuroendocrine tumors).
Management
Management of Cushing’s syndrome depends on the underlying etiology and disease severity. Optimal care often involves a multidisciplinary team comprising endocrinologists, neurosurgeons, radiologists, and sometimes oncologists.
Surgical Treatment
Transsphenoidal Resection of the Pituitary Adenoma
First-line definitive therapy for Cushing’s disease (pituitary adenoma).
Initial remission rates range from 70–90% depending on tumor size and surgical expertise.
Performed by an experienced neurosurgeon specialized in pituitary surgery.
Adrenalectomy
Unilateral adrenalectomy is indicated for adrenal adenomas or carcinomas causing Cushing’s syndrome.
Bilateral adrenalectomy is considered in severe, refractory Cushing’s disease when pituitary surgery is unsuccessful or not feasible. Patients will require lifelong glucocorticoid and mineralocorticoid replacement.
Ectopic Tumor Resection
Surgical resection or debulking of the ectopic ACTH/CRH-secreting tumor when feasible, often combined with other modalities if malignant.
Medical Therapy
Medical therapies aim to control hypercortisolism, either by inhibiting steroidogenesis or reducing ACTH secretion. These therapies can be used as a bridge to surgery, when surgery is contraindicated, or if remission is not achieved postoperatively.
Steroidogenesis Inhibitors
Ketoconazole (Nizoral)
Typical starting dose: 200 mg two to three times daily
Can be titrated up to 400–800 mg/day in divided doses
Requires monitoring of liver function tests due to hepatotoxicity risk
Metyrapone (Metopirone)
Typical starting dose: 250 mg two or three times daily
Titration up to 750–1,000 mg three times daily based on cortisol levels
May cause androgenic side effects (hirsutism, acne)
Etomidate (IV formulation)
Used in acute severe hypercortisolism or when oral therapy is not feasible
Administered under intensive monitoring, starting with low doses (e.g., 0.02–0.06 mg/kg/min)
Mitotane (Lysodren)
Adrenolytic agent used especially in adrenal carcinoma or refractory cases
Typical oral dose starts at 1–2 g/day, increased as tolerated; target levels range from 14–20 mg/L
Pituitary-Targeted Medications
Cabergoline
Dopamine agonist started at 0.5 mg twice weekly, can be titrated up to 3 mg/week or more
May yield moderate control in some patients with mild Cushing’s disease
Pasireotide (Signifor)
Somatostatin analog specifically approved for Cushing’s disease
May reduce ACTH secretion but can cause hyperglycemia
Glucocorticoid Receptor Antagonist
Mifepristone (Korlym)
Used in endogenous Cushing’s syndrome with uncontrolled hyperglycemia
Typical dose range: 300–1200 mg/day
Monitoring for signs of cortisol withdrawal and hypokalemia is essential
Radiation Therapy
Pituitary Radiation (Conventional or Stereotactic Radiosurgery)
Typically considered if surgery is not curative or if recurrence occurs postoperatively.
May take 6–24 months to achieve full biochemical remission.
Risk of hypopituitarism should be considered and monitored over time.
References
Nieman LK et al. “The Diagnosis of Cushing’s Syndrome: An Endocrine Society Clinical Practice Guideline.” J Clin Endocrinol Metab. 2008.
Newell-Price J et al. “Cushing’s Syndrome.” Lancet. 2006.
Pivonello R et al. “Medical Treatment of Cushing’s Disease: Past, Present, and Future.” J Clin Endocrinol Metab. 2015.
Written on December 22th, 2024
<
Pharmacological Management of Thyroid Disorders (Written December 23, 2024)
Thyroid disorders are classified into two broad categories: hypothyroidism (underactive thyroid function) and hyperthyroidism (overactive thyroid function). The following sections provide a hierarchical overview of common pharmacological treatments, including indications, contraindications, side effects, and other essential considerations.
Medication
Common Brand Names / Examples
Indications
Dosage
Contraindications
Side Effects
Other Considerations
Key Points
Levothyroxine (Synthetic T4)
Synthroid, Euthyrox, Tirosint
Primary hypothyroidism
Secondary (pituitary) or tertiary (hypothalamic) hypothyroidism
Typical initial dose in otherwise healthy adults: 1.6 micrograms/kg/day
Lower initial dose (25–50 mcg/day) for older adults or those with cardiovascular disease
Dose adjustments based on TSH and clinical response (reassessed every 6–8 weeks)
Untreated adrenal insufficiency
Known hypersensitivity to levothyroxine
Signs of hyperthyroidism (e.g., palpitations, tremor) if overdosed
Rare allergic reactions
Ideally taken on an empty stomach, 30 minutes to 1 hour before breakfast
Avoid co-administration with calcium, iron, or antacids within 4 hours
Monitor TSH and free T4 regularly
Gold standard for hypothyroidism therapy
Careful in patients with pre-existing cardiovascular disease
Liothyronine (Synthetic T3)
Cytomel
Short-term T3 replacement
Adjunct therapy in combination with levothyroxine for refractory cases
Initial dose: 25 mcg once daily
May be increased by 12.5–25 mcg/day every 1–2 weeks
Close monitoring of T3, TSH, and symptoms is essential
Uncorrected adrenal insufficiency
Untreated hyperthyroidism
Known hypersensitivity
Risk of hyperthyroidism with overdose
Cardiac arrhythmias, palpitations
Anxiety, insomnia
Shorter half-life and faster onset than levothyroxine
Used less frequently as monotherapy due to fluctuating hormone levels
Typically reserved for specific scenarios (e.g., myxedema coma)
Combination with T4 may be beneficial in selected patients
Natural Desiccated Thyroid (NDT)
Armour Thyroid, Nature-Throid
Hypothyroidism in select patients who prefer a natural product or have not responded optimally to synthetic T4
Often started at 30 mg (½ grain) daily, with gradual titration
Known hypersensitivity to porcine or bovine-derived products
Untreated adrenal insufficiency
Hyperthyroid symptoms if dosage is excessive
Potential variability in potency
Contains both T4 and T3 in varying ratios
Higher potential for batch-to-batch variability
Some patients report subjective improvement
Clinical guidelines generally recommend synthetic T4 due to standardization
Methimazole
Tapazole
Graves’ disease
Toxic multinodular goiter
Hyperthyroidism prior to radioactive iodine therapy or surgery
Initial dose: 15–60 mg/day in divided doses (depending on severity)
Maintenance dose: 5–15 mg/day
Known hypersensitivity
Caution in the first trimester of pregnancy (PTU is preferred)
Agranulocytosis (rare but serious)
Rash, pruritus
Hepatotoxicity (less common than PTU)
Periodically monitor complete blood count (CBC) and liver function
Avoid in first trimester of pregnancy if possible
First-line antithyroid drug for most patients with hyperthyroidism
Monitoring of TFTs guides dosage adjustments
Propylthiouracil (PTU)
Generic (often referred to as PTU)
Patients intolerant to methimazole
First trimester of pregnancy when antithyroid therapy is necessary
Initial dosage: 100–300 mg/day in divided doses
Maintenance dosage: 50–150 mg/day
Known hypersensitivity
Hepatotoxicity (Black Box Warning)
Agranulocytosis (rare)
Rash, arthralgia
Inhibits peripheral conversion of T4 to T3
Requires more frequent dosing than methimazole
Reserved for special populations (e.g., first trimester of pregnancy)
Frequent liver function monitoring is essential
Beta-Blockers (Adjunctive Therapy)
Propranolol, Atenolol
Symptomatic control in hyperthyroidism (palpitations, anxiety, tremors)
Thyrotoxic crisis (thyroid storm)
Propranolol: 10–40 mg every 6–8 hours (titration based on heart rate and symptom control)
Severe reactive airway disease (e.g., uncontrolled asthma)
Certain types of heart block
Bradycardia, hypotension
Fatigue, dizziness
Provides rapid symptomatic relief but does not alter underlying thyroid hormone production
Nonselective beta-blockers (e.g., propranolol) can reduce peripheral T4 to T3 conversion
Not curative but crucial for symptom management
Titration based on symptom control and heart rate
Potassium Iodide (Lugol’s Iodine, SSKI)
Lugol’s Iodine, SSKI
Acute management of thyrotoxic crisis
Preoperative preparation for thyroidectomy (reduces gland vascularity)
Typical regimen: 3–5 drops (each drop ~6 mg iodine) orally 3 times daily
Known hypersensitivity to iodine
Metallic taste, GI upset
Hypersensitivity reactions (rash, angioedema)
Must be given at least 1 hour after antithyroid drugs to prevent new hormone synthesis
Effectiveness may wane due to “escape” phenomenon
Temporarily inhibits thyroid hormone release
Useful for reducing vascularity of the gland pre-surgery
Radioactive Iodine (I-131)
N/A
Graves’ disease
Toxic adenoma
Multinodular goiter
Usually a single oral dose is sufficient
Some patients may require retreatment
Pregnancy and lactation (absolute contraindications)
Hypothyroidism over time (often needs levothyroxine replacement)
Mild neck tenderness
Rarely, sialadenitis
Selectively taken up by thyroid tissue, causing localized radiation damage
Radiation safety instructions are necessary (limited contact with others, especially children and pregnant individuals)
A definitive therapy for hyperthyroidism
Post-treatment hypothyroidism is common, requiring lifelong follow-up
Hypothyroidism is characterized by insufficient production of thyroid hormones. Treatment primarily involves thyroid hormone replacement to restore normal physiological levels.
1.1 Levothyroxine (Synthetic T4)
Feature
Description
Common Brand Names
Synthroid, Euthyrox, Tirosint
Dosage
Typical initial dose: 1.6 micrograms/kg/day (adults without comorbidities)
Lower initial dose (25–50 mcg/day) in older adults or those with cardiovascular disease
Indications
Primary hypothyroidism
Secondary (pituitary) or tertiary (hypothalamic) hypothyroidism
Contraindications
Untreated adrenal insufficiency
Known hypersensitivity to levothyroxine
Side Effects
Signs of hyperthyroidism if overdosed (e.g., palpitations, insomnia, tremors)
Rare allergic reactions
Other Considerations
Ideally taken on an empty stomach, 30 minutes to 1 hour before breakfast
Monitor TSH and free T4 levels at regular intervals
Avoid co-administration with calcium, iron, or antacids within 4 hours due to absorption interference
Key Points
Levothyroxine is the standard of care for hypothyroidism.
Dose adjustments are based on TSH and clinical response, typically reassessed every 6 to 8 weeks.
Careful consideration is required in patients with pre-existing heart disease.
1.2 Liothyronine (Synthetic T3)
Feature
Description
Common Brand Names
Cytomel
Dosage
Initial dose: 25 mcg once daily
May be increased by 12.5–25 mcg/day every 1–2 weeks
Indications
Short-term T3 replacement therapy
Adjunct therapy in combination with levothyroxine in certain refractory cases
Contraindications
Uncorrected adrenal insufficiency
Untreated hyperthyroidism
Known hypersensitivity
Side Effects
Risk of hyperthyroidism with overdose
Cardiac arrhythmias, palpitations
Anxiety, insomnia
Other Considerations
Has a shorter half-life and faster onset compared to levothyroxine
Used less frequently as monotherapy due to fluctuating hormone levels
Key Points
Liothyronine is typically reserved for specific clinical scenarios (e.g., myxedema coma) or when combination therapy is deemed beneficial.
Close monitoring of T3, TSH, and patient symptoms is essential.
1.3 Natural Desiccated Thyroid (NDT)
Feature
Description
Common Brand Names
Armour Thyroid, Nature-Throid
Dosage
Often started at 30 mg (1/2 grain) daily, with gradual titration
Indications
Hypothyroidism in select patients who prefer a natural product or have not responded well to synthetic T4
Contraindications
Known hypersensitivity to porcine or bovine-derived products
Untreated adrenal insufficiency
Side Effects
Potential hyperthyroid symptoms if excessive dosage is used
Variability in potency may cause fluctuating thyroid hormone levels
Other Considerations
Composed of both T4 and T3 in varying ratios
Higher potential for batch-to-batch variability
Key Points
Some patients report subjective improvement with NDT, though clinical guidelines generally recommend synthetic T4.
Uniformity of dosage can be challenging due to the animal-derived source.
Hyperthyroidism results from excessive thyroid hormone production. Treatment options include antithyroid medications, adjunctive therapies such as beta-blockers, and definitive treatments like radioactive iodine ablation or surgical thyroidectomy.
2.1 Methimazole
Feature
Description
Common Brand Names
Tapazole
Dosage
Initial dosage: 15–60 mg/day in divided doses (depending on severity)
Maintenance dosage: 5–15 mg/day
Indications
Graves’ disease
Toxic multinodular goiter
Hyperthyroidism prior to radioactive iodine therapy or surgery
Contraindications
Known hypersensitivity
Caution in first trimester of pregnancy (propylthiouracil is preferred)
Side Effects
Agranulocytosis (rare but serious)
Rash, pruritus
Hepatotoxicity (less common than with PTU)
Other Considerations
Avoid in the first trimester of pregnancy if possible
Periodically monitor complete blood count (CBC) and liver function
Key Points
Methimazole is the first-line antithyroid drug in most patients with hyperthyroidism.
Monitoring of thyroid function tests (TFTs) helps guide dosage adjustments.
2.2 Propylthiouracil (PTU)
Feature
Description
Common Brand Names
Generally referred to as PTU (generic)
Dosage
Initial dosage: 100–300 mg/day in divided doses
Maintenance dosage: 50–150 mg/day
Indications
First trimester of pregnancy when antithyroid therapy is necessary
Patients intolerant to methimazole
Contraindications
Known hypersensitivity
Side Effects
Hepatotoxicity (Black Box Warning)
Agranulocytosis (rare)
Rash, arthralgia
Other Considerations
Has additional peripheral action by inhibiting T4 to T3 conversion
Requires more frequent dosing than methimazole
Key Points
PTU is generally reserved for special populations due to the risk of severe liver injury.
Frequent monitoring of liver function tests (LFTs) is essential during therapy.
2.3 Beta-Blockers (Adjunctive Therapy)
Feature
Description
Common Agents
Propranolol, Atenolol
Dosage
Propranolol: 10–40 mg every 6–8 hours (titration based on heart rate and symptom control)
Indications
Symptomatic control in hyperthyroidism (palpitations, anxiety, tremors)
Thyrotoxic crisis (thyroid storm)
Contraindications
Severe reactive airway disease (e.g., uncontrolled asthma)
Certain types of heart block
Side Effects
Bradycardia, hypotension
Fatigue, dizziness
Other Considerations
Used for rapid symptomatic relief rather than a disease-modifying effect
Nonselective beta-blockers (e.g., propranolol) may reduce peripheral T4 to T3 conversion
Key Points
Beta-blockers are not curative but provide crucial symptomatic relief in hyperthyroidism.
Titration is based on symptom control and heart rate.
2.4 Potassium Iodide (Lugol’s Iodine, SSKI)
Feature
Description
Common Brand Names
Lugol’s Iodine, SSKI (Saturated Solution of Potassium Iodide)
Dosage
Typical regimen: 3–5 drops (each drop contains ~6 mg iodine), orally 3 times daily
Indications
Acute management of thyrotoxic crisis
Preoperative preparation for thyroidectomy (to reduce gland vascularity)
Contraindications
Known hypersensitivity to iodine
Side Effects
Metallic taste, GI upset
Hypersensitivity reactions (rash, angioedema)
Other Considerations
Must be administered at least 1 hour after antithyroid drugs to prevent incorporation of iodine into new hormone synthesis
Key Points
Potassium iodide temporarily inhibits thyroid hormone release and decreases vascularity of the thyroid gland.
Extended therapy may lose effectiveness due to thyroid “escape” phenomenon.
2.5 Radioactive Iodine (I-131)
Feature
Description
Indications
Graves’ disease
Toxic adenoma
Multinodular goiter
Mechanism
Selective uptake by thyroid tissue, causing localized radiation damage and gradual destruction of thyroid cells
Contraindications
Pregnancy and lactation (absolute contraindications)
Side Effects
Hypothyroidism over time (often requires levothyroxine replacement)
Mild neck tenderness
Rarely, sialadenitis
Other Considerations
Usually a single oral dose is sufficient, though some patients may require retreatment
Radiation safety instructions must be provided (limited contact with others, especially children and pregnant individuals)
Key Points
Radioactive iodine is a definitive therapy for hyperthyroidism.
Post-treatment hypothyroidism is common, necessitating lifelong follow-up.
Written on December 23th, 2024
<
Modern Pharmacological Obesity Treatments (Written February 19, 2025)
Recent advances in pharmacological therapy have revolutionized obesity management. Many agents initially developed for diabetes mellitus—particularly glucagon-like peptide-1 (GLP-1) receptor agonists—are now approved or utilized off-label for weight reduction. In addition, central appetite suppressants, combination therapies, and emerging agents such as dual GIP/GLP-1 receptor agonists are expanding therapeutic options. This review provides an integrated discussion of these agents, encompassing clinical indications, contraindications, routes of administration, dosage schedules, side effects, and notable brand names.
Medication & Brand
Category
Route
Typical Dosage & Duration
Mechanism of Action
Indications
Key Side Effects
Major Contraindications / Cautions
Liraglutide (Saxenda for obesity; Victoza for diabetes)
GLP-1 Receptor Agonist
SC injection
Obesity: Start 0.6 mg daily, titrate weekly to 3 mg.
Long-term use for weight management.
Enhances satiety, slows gastric emptying
Adults with BMI ≥30, or ≥27 + comorbidities
GI symptoms (nausea, diarrhea), rare pancreatitis, injection site reactions
Personal/family history of medullary thyroid carcinoma, MEN 2, hypersensitivity
Semaglutide (Wegovy For obesity; Ozempic/Rybelsus for diabetes)
GLP-1 Receptor Agonist
SC injection (Oral form for DM only)
Obesity: Start 0.25 mg weekly, titrate every 4 weeks up to 2.4 mg.
Long-term use for weight management.
Enhances satiety, slows gastric emptying
Adults with BMI ≥30, or ≥27 + comorbidities
GI symptoms (nausea, vomiting), rare pancreatitis
Personal/family history of medullary thyroid carcinoma, MEN 2, hypersensitivity
Liraglutide (Brand for obesity: Saxenda; for diabetes: Victoza)
Semaglutide (Brand for obesity: Wegovy; for diabetes: Ozempic, Rybelsus [oral form])
These agents enhance satiety, slow gastric emptying, and promote weight loss. Liraglutide is administered via subcutaneous (SC) injection daily, whereas semaglutide is typically given once weekly (SC) for obesity indications. Both are indicated for adults with a body mass index (BMI) ≥30 kg/m² or ≥27 kg/m² with weight-related comorbidities. They are contraindicated in individuals with personal or family histories of medullary thyroid carcinoma or multiple endocrine neoplasia type 2 (MEN 2). Gastrointestinal side effects are the most common.
Originally indicated for type 2 diabetes, these oral medications induce glucosuria by blocking sodium-glucose cotransporter 2 in the proximal renal tubule, leading to modest weight reduction. Though less potent for weight loss compared to GLP-1 receptor agonists, they are sometimes used off-label in overweight or obese individuals, particularly those with coexisting type 2 diabetes. Main side effects include genitourinary infections and potential volume depletion.
Dual GIP/GLP-1 Receptor Agonists
Example: Tirzepatide (Mounjaro)
Recently approved for type 2 diabetes, tirzepatide acts on both glucose-dependent insulinotropic polypeptide (GIP) and GLP-1 receptors. Clinical trials demonstrate significant weight reduction, positioning it as a promising agent for obesity management pending additional regulatory approvals. It is administered via SC injection once weekly. Side effects overlap with those of GLP-1 receptor agonists, primarily gastrointestinal symptoms.
Central Appetite Suppressants
Phentermine (Brand: Adipex-P, Lomaira)
Phentermine + Topiramate (Brand: Qsymia)
Phentermine is a sympathomimetic amine (Schedule IV controlled substance in many regions) that stimulates norepinephrine release in the hypothalamus, reducing appetite. It is typically used short-term (up to 12 weeks). Combination with topiramate, an anticonvulsant with weight-loss properties, extends the duration of use and can enhance efficacy. These oral medications are indicated for individuals with a BMI ≥30 kg/m² or ≥27 kg/m² with comorbidities. Caution is warranted in patients with cardiovascular disease and hypertension. Topiramate carries a teratogenic risk.
Non-Controlled Appetite Suppressant
Bupropion + Naltrexone (Brand: Contrave)
Combines bupropion’s inhibition of dopamine and norepinephrine reuptake with naltrexone’s opioid receptor antagonism, reducing cravings and appetite. Indicated for long-term weight management in adults with obesity or overweight plus comorbidities. Contraindications include uncontrolled hypertension, seizure disorders, and chronic opioid use. Gastrointestinal upset, insomnia, and potential elevation in blood pressure are notable side effects.
Written on February 19, 2025
Nephrology
ESRD and GFR (Written March 21, 2025)
End-stage renal disease (ESRD) represents the final, irreversible stage of chronic kidney disease (CKD), in which renal function deteriorates severely, leading to significant morbidity and mortality. The glomerular filtration rate (GFR) is a key indicator of renal function and plays a central role in diagnosing CKD, classifying its stages, and determining the appropriate timing for renal replacement therapy such as dialysis.
I. Importance of GFR in renal function assessment
GFR measures how much blood the kidneys filter per unit time, usually expressed in milliliters per minute per 1.73 m² (mL/min/1.73 m²). A lower GFR indicates reduced kidney function. Multiple equations have been developed to estimate GFR from serum creatinine, age, sex, and other variables.
Incorporates serum creatinine, age, and sex. More accurate at lower GFR levels but can underestimate kidney function in individuals with near-normal GFR.
An improved formula over MDRD, particularly in those with higher levels of kidney function, and widely recommended in clinical practice due to better accuracy across broader ranges of GFR.
Footnote: Additional adjustments for African American individuals are considered in some versions of these equations; however, these factors are not included in the above formulas, as the practice setting in Korea does not encounter such cases.
III. Classification of CKD stages by GFR
Chronic kidney disease is traditionally divided into five stages based on GFR, as shown in Table 1.
Stage
GFR (mL/min/1.73 m²)
Description
1
≥ 90
Normal or high GFR with kidney damage
2
60 – 89
Mild decrease in GFR
3a
45 – 59
Mild to moderate decrease in GFR
3b
30 – 44
Moderate to severe decrease in GFR
4
15 – 29
Severe decrease in GFR
5
< 15
Kidney failure (ESRD)
IV. Indications for dialysis
Dialysis is typically indicated at Stage 5 or ESRD (GFR < 15 mL/min/1.73 m²). However, it may be initiated sooner if severe complications appear, such as:
Intractable fluid overload or hypertension
Severe hyperkalemia (potassium imbalance)
Metabolic acidosis refractory to medical management
Stable metabolic profile with eGFR > 10 mL/min/1.73 m² and absence of uremic symptoms
Potential for reversible acute kidney injury superimposed on chronic disease
In advanced frailty, end‑stage malignancy, or severe cognitive impairment, conservative management may be preferred after shared decision‑making.
V. Practical follow‑up recommendations
Review laboratory trends at each clinical encounter, prioritizing potassium, bicarbonate, phosphorus, calcium, and hemoglobin.
Maintain meticulous fluid balance charts and daily weights to anticipate volume overload.
Refer early to a multidisciplinary kidney care team for education on modality options and access placement.
Reassess dialysis indications whenever new symptoms, laboratory instability, or eGFR < 10 mL/min/1.73 m² arise.
Document and revisit patient values and goals to align therapy with quality‑of‑life priorities.
Written on July 29, 2025
Dermatology
Seborrheic Dermatitis and Its Differential Diagnoses (Written January 7, 2025)
Seborrheic dermatitis is a chronic, relapsing inflammatory skin condition characterized by erythema, greasy scales, and pruritus. Although it is common in areas with numerous sebaceous glands (e.g., scalp, eyebrows, nasolabial folds), various other dermatological conditions can present with overlapping or similar features. A thorough knowledge of clinical presentation and access to appropriate treatment options—including local hospital products—are crucial for accurate diagnosis and management.
Seborrheic Dermatitis: Characterized by greasy scales in sebaceous-rich areas. Management centers on reducing inflammation (low- to mid-potency steroids), controlling yeast overgrowth (antifungals), and maintaining skin barrier function (moisturizers).
Differential Diagnoses:
Allergic & Irritant Contact Dermatitis: Identify and eliminate offending agents; use topical steroids or immunomodulators to control inflammation.
Atopic Dermatitis: Chronic relapsing condition with an atopic history; mainstay includes emollients and intermittent anti-inflammatory therapy.
Xerotic Eczema: Primarily dryness-driven; responds best to consistent moisturization and short steroid courses for flares.
Candidiasis: Satellite papules and moist erythema in skin folds; topical or oral antifungals as needed.
Drug Eruption & Photosensitivity: Critical to discontinue or substitute the offending drug; supportive care (topical steroids, antihistamines) may be necessary.
Condition
Key Symptoms/Signs
Commonly Affected Areas
Diagnostic Clues
Medication Options
Local Hospital Products
Dosage & Duration
Seborrheic Dermatitis
Greasy, yellowish scales or plaques
Mild to moderate erythema
Pruritus (variable intensity)
Scalp (dandruff in mild form)
Eyebrows, nasolabial folds, glabella
Behind the ears, external ear canal
Upper chest (sternal region)
Typically clinical diagnosis
Rarely requires biopsy
Must exclude psoriasis or fungal infections if atypical
Typically improves over days to weeks after drug cessation
Drug-Induced Photosensitivity
Erythema or rash resembling sunburn
Possible eczematous or urticarial lesions in sun-exposed areas
Can be intensely pruritic
Face, neck, dorsal arms, backs of hands
Any photo-exposed region
Recent history of a photosensitizing medication
Phototesting if uncertain
Discontinue or switch offending medication
Sun protection (sunscreens, protective clothing)
Topical steroids if inflammatory
DesOwen Lotion, Betavate (if inflammatory response is significant)
Improves after avoidance of photosensitizer
Continue sun protection measures indefinitely
Madecassol Powder / Combination Ointment: Often contains Centella asiatica extract and may include antibiotic components. Used primarily for wound healing, minor abrasions, and promoting epithelialization rather than for chronic inflammatory dermatoses.
Acyclovir Cream: Formulated for herpes simplex virus lesions (e.g., cold sores), not typically indicated for eczematous conditions.
HemoRex Cream: Generally indicated for hemorrhoidal symptoms (may contain local anesthetics or low-potency steroids).
LactiCare Lotion: A lactic acid–containing moisturizer, useful for xerosis, mild eczematous dermatitis, and to maintain skin hydration.
DesOwen Lotion: A low-potency topical corticosteroid (desonide 0.05%), suitable for mild inflammatory dermatoses, including mild seborrheic dermatitis, atopic dermatitis, and contact dermatitis.
Betavate: A moderate-potency topical corticosteroid (betamethasone). Used for moderate inflammatory skin conditions (e.g., more severe seborrheic dermatitis, contact dermatitis, or psoriasis).
Silkron-G Cream: Often a combination product (e.g., steroid + antibiotic + antifungal). Used cautiously for mixed or uncertain infections, but prolonged use is discouraged without proper diagnosis.
Mujonal Cream: Typically an antifungal cream (ingredient may vary). Used for candidiasis, tinea infections, or seborrheic dermatitis of fungal etiology.
Esroban Ointment: Equivalent to mupirocin ointment in many formulations. Used for localized bacterial skin infections.
Nitrofurazone Ointment: An antibacterial product. Often for burns or superficial infections.
Silver Sulfadiazine (Silmazine): Commonly used for burns to prevent and treat infections.
Endix Ointment: May contain antibiotic or combination components—used for superficial bacterial skin infections.
Written on January 7, 2025
Radiology
Pending CXR Examination (Written December 25, 2024)
1. Possible Phrasings
Formal & Detailed:
CXR imaging has not been performed by the radiologic technologist as of 2024-12-25, despite being requested on 2024-12-06.
Concise:
CXR remains unperformed as of 2024-12-25, requested on 2024-12-06.
Brief:
CXR pending since 2024-12-06.
CXR pending from 12/6 to 12/25.
Imaging pending until 12/25.
2. Notes
Dates: Clearly list both the request date and the current/pending date.
Responsible Party: Specify “radiologic technologist” (or equivalent) when relevant.
Tone: Maintain professionalism by stating facts objectively.
Consistency: Use similar phrasing across the patient record for clarity.
Choose the most suitable option based on the context and required level of de
Written on December 25th, 2024
Cross-Sectional Imaging Techniques for the Thorax (Written January 8, 2025)
Cross-sectional imaging has revolutionized thoracic diagnostics by providing detailed visualization of the lungs, mediastinum, vascular structures, and surrounding tissues. Common modalities include Computed Tomography (CT), Magnetic Resonance Imaging (MRI), and Ultrasound (US). Each modality has specific strengths, limitations, and optimal clinical applications. This document presents an integrated discussion of imaging planes, image interpretation, characteristic features of different modalities, and considerations for selecting the best imaging technique.
Parameter
CT
MRI T1-Weighted
MRI T2-Weighted
Ultrasound
Key Indications
Pulmonary nodules, masses, infections
Trauma evaluation (chest wall, lung)
Pulmonary embolism (CTPA)
Anatomical detail (chest wall, mediastinal fat)
Post-contrast imaging (gadolinium)
Fluid collections (effusions, cysts)
Inflammatory or edematous changes
Assessing pleural effusions, empyemas
Guidance for fluid drainage
Advantages
Fast acquisition, high spatial resolution
3D reconstructions
Excellent for demonstrating fat and soft tissue interfaces
Better anatomical contrast than CT for certain tissues
Highly sensitive to fluid, edema, and inflammation
Cine imaging for dynamic motion (cardiac)
No radiation
Portable and real-time
Limitations
Ionizing radiation
Iodinated contrast risks
Longer scan times
Costly and less available than CT
Susceptible to motion artifacts
Not all patients tolerate MRI environment
Limited penetration through air or bone
Operator-dependent
Contraindications / Cautions
Pregnancy (relative; avoid if possible)
Severe renal insufficiency (contrast studies)
Metallic implants, pacemakers
Claustrophobia
Same as T1 (MRI environment restrictions)
Gadolinium caution in renal failure
Bone or air-filled areas limit utility
Obesity can reduce image quality
Imaging Planes: Axial, Sagittal, Coronal, and Oblique
Axial (Transverse) Plane
Oriented horizontally, dividing the body into superior (upper) and inferior (lower) parts.
Chest CT images are conventionally viewed as if looking up from the patient’s feet (i.e., from below). The patient’s right side appears on the left side of the image.
Sagittal Plane
Divides the body into right and left portions.
Useful for assessing anterior-to-posterior relationships within the thorax, such as the position of mediastinal masses relative to the sternum or vertebral column.
Coronal Plane
Splits the body into anterior (front) and posterior (back) segments.
Aids in evaluating the lungs and mediastinal structures in a frontal perspective.
Oblique Plane
Any plane that deviates from the standard axial, sagittal, or coronal orientations.
Employed to better delineate lesions or structures that follow complex trajectories (e.g., vascular or bronchial abnormalities).
Computed Tomography (CT) of the Chest
Basic Principles
CT imaging uses X-rays and computer processing to generate cross-sectional slices. Structures can be evaluated based on their Hounsfield Unit (HU) measurements, which quantify tissue density.
Hounsfield Scale (Approximate Ranges)
Tissue / Structure
HU Value
Comments
Air (e.g., pneumothorax)
~ –1000
Most radiolucent
Lung Parenchyma
~ –800
Varies with inflation and pathology
Fat
~ –80 to –120
Subcutaneous or mediastinal fat
Water
0
Reference point
Muscle
~ +40
Soft tissue density
Bone
~ +350 (can range +300 to +1000)
Highly radiodense
Higher HU values indicate denser (more radiopaque) tissues (e.g., bone).
Lower (negative) HU values represent radiolucent (less dense) tissues or air (e.g., lung, pneumothorax).
Bone Window: Enhances bony detail for detecting rib fractures or focal lesions in vertebrae.
Advantages of CT
Rapid imaging with high spatial resolution, ideal for evaluating lung parenchyma, pleural abnormalities, and acute chest conditions.
Widely available and relatively straightforward to perform in most clinical settings.
Enables three-dimensional reconstructions for surgical planning or further analysis.
Disadvantages of CT
Ionizing Radiation exposure.
Frequent use of iodinated contrast agents, which may pose risks for nephrotoxicity or allergic reactions in susceptible individuals.
Common Indications and Contraindications for Chest CT
Indications
Contraindications / Cautions
Detection and characterization of pulmonary nodules, masses, or infections
Evaluation of pulmonary embolism (CT pulmonary angiogram)
Assessment of traumatic injuries to the chest wall, lungs, or mediastinum
Preoperative mapping for thoracic surgery
Severe contrast allergy or renal insufficiency (when contrast is indicated)
Concerns about radiation dose in pregnant patients or pediatric populations
Need to avoid iodinated contrast in hyperthyroidism or specific drug interactions
Magnetic Resonance Imaging (MRI) of the Chest
Basic Principles
MRI relies on the interaction of hydrogen nuclei with strong magnetic fields and radiofrequency pulses. Different pulse sequences emphasize various tissue properties such as fat, fluid, and blood flow. Unlike CT, MRI does not use Hounsfield Units; instead, tissue characterization is based on signal intensities, primarily determined by T1 and T2 relaxation times.
Characterizing cystic lesions or pleural effusions
Contrast Agents and Safety Considerations
Gadolinium-Based Contrast Materials: Used to enhance vascularity and tissue perfusion in MRI.
Advantages of MRI include the absence of ionizing radiation and avoidance of iodinated contrast, reducing certain risks associated with CT. However, gadolinium agents can be contraindicated in patients with severe renal dysfunction due to the risk of nephrogenic systemic fibrosis.
Indications and Contraindications for Chest MRI
Indications
Contraindications / Cautions
Cardiac imaging: functional assessment of the heart in systole and diastole
Vascular and mediastinal tumors: delineation of vascular invasion and soft tissue detail
Assessment of complex chest wall or spinal involvement (e.g., Pancoast tumors)
Further characterization of indeterminate soft tissue lesions
Presence of certain metallic implants, pacemakers, or devices incompatible with strong magnetic fields
Claustrophobia or inability to remain still (though sedation or open MRI scanners may mitigate these issues)
Renal insufficiency when using gadolinium-based agents
Ultrasound (US) of the Chest
Role of Ultrasound
Ultrasound is less commonly employed for routine lung imaging because air-filled lung parenchyma impedes sound wave transmission. However, it is highly valuable for pleural assessments and other specific thoracic applications.
Evaluating Pleural Effusions and Empyema
Ultrasound can differentiate transudates vs. exudates by comparing echogenicity relative to the liver or spleen.
Transudates often appear anechoic or hypoechoic (similar or slightly darker than liver).
Exudates or empyemas may show internal echoes, septations, or debris, indicating higher protein or cellular content.
Real-time guidance for thoracentesis or drainage makes ultrasound indispensable in managing pleural fluid collections.
Advantages and Limitations
Advantages: No radiation, real-time imaging, portability (e.g., bedside use), excellent for fluid assessment and guided interventions.
Limitations: Air in the lungs and bony structures limit visualization of deeper thoracic structures.
Best Imaging Modality for Specific Clinical Scenarios
Pleural Effusion
Ultrasound is highly sensitive for detecting and characterizing pleural fluid, guiding thoracentesis, and differentiating between transudates and exudates.
Tumor Invading the Mediastinum
MRI is often preferred for superior soft tissue delineation and assessment of tumor invasion into mediastinal structures, major vessels, or the spine.
Assessment of Heart in Systole and Diastole
MRI offers detailed cine sequences to visualize cardiac function dynamically.
CT can provide gated images of the heart but typically relies on rapid data acquisition rather than continuous real-time evaluation.
Written on January 7, 2025
Differentiating Alveolar and Interstitial Changes in General (Written January 8, 2025)
Understanding the distinction between alveolar (often referred to as radiolucent under normal conditions but appearing radiodense when filled with fluid or exudate) and interstitial (commonly described as radiodense when thickened) lung changes is essential in interpreting chest imaging findings and guiding clinical management. Alveolar and interstitial patterns manifest differently on radiographs or computed tomography (CT) scans and are associated with distinct pathological processes, most notably alveolar pneumonia vs. interstitial pneumonia or alveolar consolidation vs. interstitial thickening.
Feature
Alveolar (Airspace) Pattern
Interstitial Pattern
Appearance on X-ray/CT
Fluffy, confluent opacities; air bronchograms
Linear, reticular, or reticulonodular markings
Primary Location
Alveolar spaces filled with exudate/fluid
Alveolar walls, septa, connective tissue
Radiodensity
Radiodense when alveolar spaces are filled
Radiodense lines or nets within lung interstitium
Clinical Examples
Lobar pneumonia, pulmonary edema, hemorrhage
Interstitial pneumonia, pulmonary fibrosis, edema
Onset
Often acute
Often subacute or chronic
Typical Symptoms
Productive cough, acute fever, localized signs
Progressive dyspnea, dry cough, diffuse findings
I. Alveolar Region and Alveolar (Airspace) Changes
Normal Appearance of Alveoli
The alveoli are typically air-filled, creating a radiolucent appearance on standard chest radiographs.
Under normal conditions, the alveolar walls and spaces are not individually visible because of their thin structure and the dominance of air.
Alveolar (Airspace) Opacification
When alveoli become filled with fluid, pus, blood, or cells (e.g., in pneumonia, hemorrhage, or edema), they appear more radiodense (opaque) on imaging.
Alveolar opacification often presents as fluffy, confluent, or homogeneous densities that may obscure normal anatomic landmarks, such as vascular markings or airway outlines.
Alveolar Pneumonia (Consolidation)
Pathophysiology: Characterized by an infectious or inflammatory process within the alveolar spaces. Exudate accumulates in the alveoli, reducing air content and increasing radiodensity on imaging.
Radiological Features:
Homogeneous or segmental consolidations.
Air bronchograms (air-filled bronchi made visible by surrounding alveolar opacification).
Clinical Correlation: Often presents with acute symptoms (fever, productive cough, and localized auscultatory findings).
Alveolar Consolidation
Definition: Consolidation refers to the filling of alveolar spaces with fluid or cells, leading to increased density.
Imaging Appearance:
Lobar or segmental distribution of opacities.
Tendency to have clearly demarcated borders correlating with anatomical lung segments.
II. Interstitial Region and Interstitial (Supporting Framework) Changes
Normal Interstitium
The interstitium consists of alveolar septa, connective tissue, and the supporting framework of the lung.
Under normal conditions, it contributes subtle linear markings without forming dense, reticular, or nodular patterns on standard chest radiographs.
Interstitial Thickening (Radiodense)
Thickening or infiltration of the interstitial tissues (by fluid, fibrosis, or inflammatory cells) increases radiodensity in a linear, reticular, or reticulonodular pattern.
Unlike alveolar consolidation, the airspace is generally preserved, so air bronchograms are less common.
Interstitial Pneumonia
Pathophysiology: Involves inflammation primarily within the interstitial and alveolar wall regions rather than the alveolar spaces.
Radiological Features:
Reticular or reticulonodular markings.
Ground-glass opacities on CT scans.
More diffuse involvement, often bilateral, reflecting widespread interstitial inflammation.
Clinical Correlation: Symptoms may be more chronic or subacute (e.g., progressive dyspnea, a dry cough, and diffuse auscultatory findings).
Interstitial Thickening
Definition: Thickening of alveolar septa or interstitial tissues by edema, fibrotic changes, or infiltration.
Imaging Appearance:
Linear septal lines (Kerley B lines).
Ground-glass changes on high-resolution CT.
“Honeycombing” in fibrotic conditions.
III. Clinical and Diagnostic Implications
Alveolar Pneumonia vs. Interstitial Pneumonia
Alveolar pneumonia: Typically caused by bacteria (e.g., Streptococcus pneumoniae) presenting with lobar consolidation and acute symptoms.
Interstitial pneumonia: More commonly associated with viruses, atypical bacteria, or chronic processes (e.g., Mycoplasma, fungi, or idiopathic pulmonary fibrosis), presenting with a more gradual onset.
Alveolar Consolidation vs. Interstitial Thickening
Alveolar consolidation: Rapidly developing opacities that can obscure vascular markings, often associated with exudative processes.
Interstitial thickening: Progressive radiodensities in linear or reticular patterns suggesting fibrosis or infiltrative disease.
Treatment Considerations
Alveolar (Consolidation) Processes: Require treatments targeting the cause (e.g., antibiotics for bacterial pneumonia, diuretics for edema).
Interstitial Processes: Often managed with anti-inflammatory agents (corticosteroids), immunosuppressants, or supportive measures, depending on the underlying etiology.
Prognostic Differences
Alveolar disorders can often resolve completely if treated appropriately.
Interstitial disorders (particularly fibrotic changes) may result in permanent structural lung alterations if not addressed early.
Written on January 7, 2025
Radiographic Differentiation of Interstitial and Alveolar Lung Diseases (Written January 8, 2025)
Lung parenchyma is broadly divided into two key components: the interstitium (supporting structures such as arteries, veins, and bronchi) and the alveoli (air sacs). On a normal chest radiograph (CXR), these structures manifest distinct appearances that help differentiate various pulmonary pathologies—primarily interstitial lung disease versus alveolar (airspace) filling disease.
Normal Lung Anatomy and Radiographic Appearance
Interstitium
Composed of the supporting vasculature (arteries and veins), bronchi, and connective tissue.
On a normal CXR, the branching pulmonary vessels appear prominent near the hilum but diminish in caliber peripherally, eventually disappearing beyond the resolution of the X-ray beam.
Alveoli
Tiny air-filled sacs where gas exchange occurs.
Individually too small to visualize on CXR; collectively render the lung fields radiolucent (dark) under normal aeration.
Normal Radiographic Signs
The interstitial markings gradually fade outward.
The alveoli are uniformly aerated, imparting a clear, lucent appearance.
The diaphragms are typically seen at the 9th to 10th posterior rib level on full inspiration.
Feature
Interstitial Disease
Alveolar (Airspace) Filling Disease
Visibility of Pulmonary Vessels
Prominent, often more numerous or distorted
Diminished or obscured within the consolidated areas
Lung Aeration
Maintained (alveoli remain air-filled)
Reduced or absent in involved regions (alveoli filled with fluid)
Air Bronchogram
Rarely visible
Often present (unless bronchi are also filled with fluid)
Silhouette Sign
Not typical, as aerated lung usually surrounds vessels and mediastinal borders
Common, especially if consolidation abuts the heart, diaphragm, or aortic arch
Disease Pattern
Reticular, nodular, or reticulonodular; in chronic cases, shows distortion or honeycombing
Homogeneous or patchy consolidation, may exhibit air bronchograms and silhouette sign
Interstitial Lung Disease
Thickening or alteration of the supporting structures (bronchi, vessels, connective tissue) while alveoli typically remain aerated. Lungs appear aerated, yet pulmonary markings are increased in number, prominence, or distortion.
Acute vs. Chronic Interstitial Disease
Acute Interstitial Changes:
Markings appear hazy or ill-defined.
No significant angular or irregular distortions of vessels.
Chronic Interstitial Changes:
Markings are sharp, well-defined, and distorted (e.g., angular, bowed, or irregular).
May exhibit characteristic findings such as honeycombing or other fibrotic patterns.
Types of Interstitial Patterns
Reticular (Linear) Pattern
Appears as a network of fine lines.
May progress to coarse reticulation or honeycombing in chronic stages.
Nodular Pattern
Manifests as discrete nodular densities scattered throughout the lungs.
Can be focal, multifocal, or diffuse.
Reticulonodular Pattern
Combination of both linear and nodular changes.
Silhouette and Air Bronchogram in Interstitial Disease
Silhouette Sign: Typically absent because aerated alveoli remain interposed between pulmonary vessels and adjacent structures (e.g., diaphragm, heart, aorta).
Air Bronchogram: Rarely seen, since the bronchi are still surrounded by aerated lung tissue.
Alveolar (Airspace) Filling Disease
Filling of alveoli by fluid, exudate, or other material, replacing the normal air content. Portions of the lung appear opaque, obscuring the underlying vascular markings in those areas.
Radiographic Characteristics
Reduced Visibility of Vessels in the consolidated regions.
Homogeneous or Patchy Opacification indicating alveolar filling.
Air Bronchogram Sign
Often present because bronchi remain air-filled while the surrounding alveoli are opacified with fluid/disease.
Absent if the bronchi themselves are also filled with fluid.
Silhouette Sign
Present when consolidated (water-density) alveoli are in direct contact with adjacent water-density structures (e.g., heart border, diaphragm, aorta).
Absent if the consolidation does not physically contact a structure of similar density.
Multifocal Alveolar Disease
Small, multiple areas of alveolar consolidation may not consistently demonstrate air bronchograms (especially if bronchi are filled or if the area of consolidation is too small). The silhouette sign appears only when consolidation abuts a known anatomical border.
Key Radiographic Signs
Silhouette Sign
Loss of the normal interface between the lung and adjacent structures when both become the same radiographic density.
Typical of alveolar consolidation abutting the heart border, diaphragm, or aortic knob.
Rare in interstitial disease because some aerated lung typically remains at the interface.
Air Bronchogram
Visualization of air-filled bronchi within an opaque (consolidated) lung field.
Characteristic of alveolar filling disease when bronchi remain patent.
Uncommon in interstitial disease because surrounding alveolar spaces are still air-filled.
Hyperinflation
Diaphragms appear flattened and depressed to or below the 10th posterior rib.
Often noted in emphysema, sometimes accompanied by visible bullae (lucent areas devoid of normal lung markings).
Additional Considerations
Assessing Chronicity: Comparison with prior radiographs is often the most reliable indicator of disease progression or chronicity.
Honeycombing: Sign of advanced fibrotic change in chronic interstitial processes.
Distortion of Markings: Another hallmark of chronic interstitial disease.
Multifocal Alveolar Infiltrates: May not produce a classic air bronchogram if bronchi are obstructed or if the affected areas are too small or widely scattered.
Written on January 8, 2025
Radiographic Features of Interstitial and Alveolar Pneumonia (Written January 8, 2025)
This document provides a comprehensive overview of the characteristic chest X-ray (CXR) findings associated with interstitial and alveolar pneumonia, along with guidance on interpreting related radiological terminology. The purpose is to offer a refined, systematic, and professional reference for clinicians and radiologists.
Feature
Alveolar Pneumonia
Interstitial Pneumonia
Primary Radiographic Pattern
Homogeneous or patchy alveolar opacities (consolidation, air bronchograms, silhouette sign)
Reticular, nodular, or reticulonodular changes (septa thickening, fine linear densities)
Lung Volumes
May be reduced in severe consolidation
Often preserved, even if opacities are present
Terminology Clues
“Increased infiltration and consolidation” → alveolar filling
“Increased radiopacity” in a diffuse, lattice-like or nodular fashion → interstitial involvement
Alveolar Pneumonia
Alveolar pneumonia involves the airspaces (alveoli) becoming filled with fluid, inflammatory cells, or exudates. On CXR, this process typically presents as more homogeneous or patchy opacities, often with characteristic signs such as air bronchograms or silhouette signs.
Lobar Consolidation
Dense homogeneous opacity in the right lower lobe, obliterating the right hemidiaphragm contour, consistent with alveolar consolidation.
A well-demarcated, dense opacity that replaces air in the affected lobe, frequently obscuring adjacent anatomical borders.
Patchy Airspace Opacities
Bilateral patchy alveolar infiltrates with air bronchograms, more pronounced in the mid-lung fields, suggestive of multifocal pneumonia.
Patchy areas of increased density with visible air-filled bronchi (air bronchograms) are typical of alveolar filling processes.
Silhouette Sign
Ill-defined opacity in the left lower zone obscuring the left heart border, indicating alveolar involvement with a positive silhouette sign.
The loss of the normal interface between the lung and adjacent structures (e.g., heart border or diaphragm) supports alveolar consolidation in that region.
Interstitial Pneumonia
Interstitial pneumonia primarily involves the interstitial structures of the lung, such as the alveolar septa and the interlobular septa. On CXR, the hallmark is a reticular, nodular, or reticulonodular pattern rather than dense, homogeneous opacities.
Diffuse Reticular Pattern
Bilateral fine reticular opacities predominantly in the lower zones, with preserved lung volumes, suggestive of an interstitial process.
This description underscores subtle, thread-like opacities extending across both lungs, often sparing normal lung volumes.
Septal Thickening
Prominent interlobular septal lines and mild perihilar reticulation, consistent with an interstitial pneumonia pattern.
Thickening of the septa creates linear densities throughout the lung fields, reflecting an underlying interstitial process.
Reticulonodular Opacities
Diffuse reticulonodular opacities without significant consolidation; interstitial pneumonia should be considered.
A combination of fine linear and nodular lesions scattered throughout the lung parenchyma suggests the possibility of interstitial pneumonia.
Radiographic Terminology
Increased Infiltration
Refers to the filling of alveolar spaces by fluid, exudate, or cells, commonly encountered in alveolar processes such as pneumonia or pulmonary edema.
Typically associated with alveolar processes.
Increased Radiopacity
Alveolar Pattern: Radiopacity arises from replacement of air in the alveoli by fluid, pus, or blood, creating dense or homogeneous opacities (e.g., lobar consolidation).
Interstitial Pattern: Radiopacity results from thickening of interstitial structures (e.g., alveolar septa, interlobular septa, or fibrosis). This manifests as reticular, nodular, or reticulonodular patterns rather than consolidated, uniform opacities.
Radiographic Findings in a General Way
Alveolar Pneumonia
The chest X-ray reveals regions of increased density in the lung tissue, which may suggest that fluid, pus, or inflammatory material has filled the airspaces.
There are patchy areas of consolidation observed on the image, consistent with an alveolar infection.
Some areas of the lung show a loss of normal boundaries with adjacent structures, often seen when dense inflammatory material is present.
Interstitial Pneumonia
The imaging displays a network-like or lattice pattern throughout the lungs, which can be indicative of inflammation or scarring within the lung’s supporting framework.
Instead of large consolidated areas, the X-ray shows a diffuse web of linear and small nodular opacities, suggesting changes in the lung interstitium.
A subtle, widespread pattern of increased markings is evident, pointing to interstitial lung disease.
Approximate pleural effusion volume on chest X-ray (upright PA) — rough reference (Written February 23, 2026)
I. Upright PA reference ranges
Costophrenic angle (CPA) blunting: ~200–300 mL
Clear meniscus sign: ~300–500 mL
Effusion occupying ~1/3 of a hemithorax: ~500–1000 mL
Near-complete hemithorax opacification: >1000–1500 mL
Pharmacologic Agents and Interventional Procedures (Written December 22, 2024)
Table of Contents
Introduction
Pharmacologic Interventions
Local Anesthetics – Lidocaine
Corticosteroids – Triamcinolone and Dexamethasone
Interventional Procedures
Nerve Block
C-arm Guided Nerve Blocks
Radiofrequency Ablation
Shockwave Therapy
Comparative Summary Table
Expanded Procedural Guidelines
Lidocaine Injection Technique
Corticosteroid Injection Technique
Nerve Block Technique
C-arm Guided Nerve Blocks
Radiofrequency Ablation Essentials
Shockwave Therapy Key Steps
Conclusion
1. Introduction
Pain management frequently requires a comprehensive approach that may include local anesthetics, corticosteroids, nerve blocks, radiofrequency ablation (RFA), and shockwave therapy. Each modality provides distinct mechanisms of action, has specific indications and contraindications, and carries potential complications. When appropriately selected and administered, these interventions can offer substantial relief from acute or chronic pain.
A careful review of each treatment’s pharmacodynamics, procedural protocols, and potential adverse effects informs responsible clinical decision-making. Imaging techniques—such as ultrasound or fluoroscopy—further enhance safety and accuracy, helping ensure optimal patient outcomes.
2. Pharmacologic Interventions
2.1 Local Anesthetics – Lidocaine
Mechanism of Action
Blocks sodium channels, preventing the propagation of action potentials along nerve fibers. This effect produces temporary loss of sensation or pain relief in the targeted area.
Indications
Acute musculoskeletal pain.
Diagnostic nerve blocks (for delineating the pain source).
Minor surgical procedures (e.g., superficial excisions, suturing).
Contraindications
Known allergy (hypersensitivity) to amide-type local anesthetics.
Local infection at the injection site.
Dosage & Preparation
Concentration: Commonly 1% (10 mg/mL). If 2% solution (20 mg/mL) is used, dilute it 1:1 with normal saline to obtain 1%.
Volume: Typically 1–10 mL, depending on the target site and size of the area.
Needle Gauge: 22–25 G for superficial or peripheral blocks; 20–22 G for deeper or larger joints.
Procedure Considerations
Employ sterile technique and aspirate before injection to avoid intravascular placement.
Consider the addition of epinephrine (1:100,000) to prolong anesthetic effect, unless injecting into end-arterial sites such as digits or the penis.
Monitor for systemic toxicity (e.g., perioral numbness, tinnitus, metallic taste), especially with larger volumes.
Systemic: Hyperglycemia, edema, Cushingoid changes, adrenal suppression with repeated use.
3. Interventional Procedures
3.1 Nerve Block
Definition
A nerve block involves injecting local anesthetics (often combined with corticosteroids) around or near a specific nerve or nerve bundle to interrupt nociceptive signals. This technique may be diagnostic (to confirm the nerve's role in pain generation) or therapeutic (to provide intermediate or long-term relief).
Indications
Acute musculoskeletal pain, neuropathic pain, or mixed etiologies.
Diagnostic assessment to identify pain sources (e.g., facet vs. sacroiliac vs. peripheral nerve entrapment).
Contraindications
Local infection at the injection site.
Coagulopathy or anticoagulant therapy (relative contraindication).
Known allergy to injectate components.
Procedure Steps
Localization: Ultrasound guidance or a nerve stimulator is employed to identify the target nerve accurately.
Needle Gauge: Typically 22–25 G for peripheral blocks; 18–22 G for deeper or epidural-type procedures.
Injectate: 1–2% Lidocaine or 0.25–0.5% Bupivacaine, optionally combined with a low dose of corticosteroid (e.g., Dexamethasone 1–4 mg).
Volume: Generally 5–10 mL for peripheral nerve blocks, adjusted based on the nerve's location and the tissue space.
Aspirate: Frequent aspiration before each incremental injection is essential to avoid intravascular injection.
Potential Complications
Neurological: Nerve injury, transient numbness or paresthesia.
Systemic: Local anesthetic systemic toxicity (LAST) if accidental intravascular administration occurs.
Others: Hematoma, infection, allergic reaction.
3.1.1 C-arm Guided Nerve Blocks
Definition
C-arm guided nerve blocks utilize fluoroscopic imaging to enhance the precision of nerve localization and injectate placement. The C-arm provides real-time X-ray imaging, allowing for accurate needle positioning relative to bony landmarks and soft tissues.
Indications
Nerve blocks requiring precise anatomical localization, such as epidural, facet joint, or sacroiliac joint blocks.
Patients with complex anatomy where ultrasound guidance may be challenging.
Procedures where bony landmarks are essential for accurate placement.
Contraindications
Allergy to contrast media, if contrast is used.
Pregnancy, due to radiation exposure (relative contraindication).
Severe obesity or inability to obtain clear fluoroscopic images.
Procedure Steps
Preparation: Ensure the availability of fluoroscopic equipment (C-arm) and necessary shielding to protect patient and staff from radiation.
Patient Positioning: Position the patient appropriately based on the target nerve block, ensuring comfort and access to the injection site.
Imaging Setup: Adjust the C-arm to obtain the necessary fluoroscopic views (anteroposterior, lateral, oblique) for accurate needle placement.
Needle Insertion: Insert the needle under continuous fluoroscopic visualization, advancing it towards the target nerve or joint space.
Confirmation: Inject a small amount of contrast dye to verify correct placement of the injectate around the target area.
Administration of Injectate: Once proper placement is confirmed, administer the prescribed local anesthetic and/or corticosteroid.
Final Imaging: Perform a final fluoroscopic check to ensure there is no unintended spread of the injectate.
Potential Complications
Radiation Exposure: Both patient and clinician are exposed to ionizing radiation; minimize exposure by using appropriate shielding and limiting fluoroscopy time.
Infection: Risk of introducing pathogens during needle insertion; strict aseptic technique is mandatory.
Bleeding: Potential for hematoma formation, especially in patients with coagulopathy.
Nerve Injury: Risk of direct trauma to nerves or adjacent structures.
Contrast Reaction: If contrast media is used, there is a risk of allergic reactions or nephropathy in susceptible individuals.
Procedure Considerations
Use appropriate radiation protection measures, including lead aprons, thyroid shields, and minimizing fluoroscopy time.
Ensure clear identification of anatomical landmarks using fluoroscopic images.
Consider using contrast agents to verify injectate placement, especially in complex or deep structures.
3.2 Radiofrequency Ablation
Mechanism of Action
Radiofrequency Ablation (RFA) uses thermal energy (often 80–90°C for 60–90 seconds) to create a lesion on specific sensory nerves, thereby interrupting pain transmission for an extended period.
Indications
Chronic facet (zygapophyseal) joint pain in the lumbar or cervical spine.
Sacroiliac joint pain, genicular nerve pain in the knee when diagnostic nerve blocks confirm the nerve’s involvement in pain.
Contraindications
Active local infection.
Coagulopathy or bleeding disorders.
Pregnancy (relative contraindication, especially if exposing the patient to fluoroscopy).
Procedure Steps
Imaging Guidance: Fluoroscopy or ultrasound used to guide the specialized RFA needle (often 18–22 G) into the correct position.
Confirmation: Sensory and motor stimulation tests confirm accurate nerve targeting before ablation.
Thermal Lesioning: Usually 80–90°C for 60–90 seconds to maximize denervation of the sensory branch.
Analgesia/Sedation: Local anesthesia and mild sedation may be provided for patient comfort.
Potential Complications
Local Tissue Injury: Excessive heat may damage adjacent structures, though precisely controlled temperature reduces this risk.
Nerve Injury: Potential for neuritis or neuropathic pain.
Infection or Hematoma: Risk is minimized by sterile technique and careful patient selection.
Duration of Relief
Pain relief may last from 6 to 12 months. Repeated RFA is possible if symptoms recur.
3.3 Shockwave Therapy
Mechanism of Action
Delivers high-energy acoustic waves that stimulate microtrauma in musculoskeletal tissues, enhancing tissue repair and providing analgesic effects.
Indications
Chronic tendinopathies, such as plantar fasciitis, rotator cuff calcific tendonitis, and epicondylitis.
Myofascial pain syndromes.
Contraindications
Open growth plates, acute fractures, malignancy in the treatment area.
Severe coagulopathy.
Procedure Steps
Application: A handheld shockwave applicator delivers pulses through ultrasound gel on the skin overlying the affected structure.
Treatment Protocol: Typically 3–6 sessions spaced 1–2 weeks apart, with incremental increases in energy based on patient feedback.
Patient Sensation: Some discomfort may occur; energy levels can be adjusted accordingly.
Potential Complications
Localized bruising, transient swelling, or increased pain (flare) in the treated site.
Rare tendon or ligament injury if excessive energy is delivered.
4. Comparative Summary Table
Intervention
Mechanism
Primary Indications
Contraindications
Dosage / Administration
Key Procedure Tips
Potential Complications
Lidocaine
Sodium channel blockade for local anesthesia
Acute musculoskeletal pain, minor procedures, nerve blocks
Amide local anesthetic allergy; infection at site
Concentration: 1% (dilute 2% if necessary) Volume: 1–10 mL Needle Gauge: 22–25 G (or 20–22 G for deeper)
Open growth plates, acute fractures, malignancy, coagulopathy
Sessions: 3–6, spaced 1–2 weeks apart Energy Level: Increased gradually by tolerance
Precise probe positioning
Use ultrasound gel
Adjust frequency/energy for patient comfort
Bruising, transient pain flare
Rare tendon/ligament injury if improperly applied
5. Expanded Procedural Guidelines
5.1 Lidocaine Injection Technique
Preparation of 1% Lidocaine
If only 2% lidocaine is available (20 mg/mL), dilute with an equal volume of normal saline.
Example: 5 mL of 2% lidocaine + 5 mL of normal saline = 10 mL of 1% solution.
Aspiration
Before injecting, aspirate to reduce the risk of intravascular placement.
Monitoring
Watch for early signs of toxicity (e.g., metallic taste, tinnitus, lip tingling).
5.2 Corticosteroid Injection Technique
Triamcinolone
Dose ranges from 10–40 mg per injection, depending on the targeted joint’s size.
Consider combining with lidocaine to alleviate discomfort and provide immediate analgesia.
Dexamethasone
Typically administered in doses of 1–4 mg for small joints or epidural injections.
Imaging guidance (fluoroscopy for epidurals, ultrasound for joints) is strongly recommended.
5.3 Nerve Block Technique
Localization
Ultrasound visualization or a peripheral nerve stimulator to confirm target nerve.
Injectate
1–2% Lidocaine or 0.25–0.5% Bupivacaine with or without a low-dose corticosteroid.
Incremental Injection
Incrementally inject, aspirating before each aliquot to prevent intravascular injection.
Observation
Monitor for local anesthetic systemic toxicity and neurological changes.
5.3.1 C-arm Guided Nerve Blocks
Preparation
Ensure the availability of fluoroscopic equipment (C-arm) and necessary radiation shielding for patient and staff.
Patient Positioning
Position the patient based on the target nerve block, ensuring optimal access and comfort.
Imaging Setup
Adjust the C-arm to obtain the required fluoroscopic views (anteroposterior, lateral, oblique) to accurately localize the target nerve or joint space.
Needle Insertion
Insert the needle under continuous fluoroscopic guidance, advancing towards the target nerve or joint space while avoiding critical structures.
Confirmation
Inject a small amount of contrast dye to verify correct placement of the injectate around the target area.
Administration of Injectate
Once proper placement is confirmed, administer the prescribed local anesthetic and/or corticosteroid.
Final Imaging
Perform a final fluoroscopic check to ensure there is no unintended spread of the injectate.
Potential Complications
Radiation Exposure: Both patient and clinician are exposed to ionizing radiation; minimize exposure by using appropriate shielding and limiting fluoroscopy time.
Infection: Risk of introducing pathogens during needle insertion; strict aseptic technique is mandatory.
Bleeding: Potential for hematoma formation, especially in patients with coagulopathy.
Nerve Injury: Risk of direct trauma to nerves or adjacent structures.
Contrast Reaction: If contrast media is used, there is a risk of allergic reactions or nephropathy in susceptible individuals.
Procedure Considerations
Use appropriate radiation protection measures, including lead aprons, thyroid shields, and minimizing fluoroscopy time.
Ensure clear identification of anatomical landmarks using fluoroscopic images.
Consider using contrast agents to verify injectate placement, especially in complex or deep structures.
5.4 Radiofrequency Ablation (RFA) Essentials
Probe Placement
Use fluoroscopy or ultrasound to accurately position the RFA cannula.
Confirmation Testing
Apply sensory and motor stimulation to confirm accurate target nerve placement before ablation.
Lesioning
Usually performed at 80–90°C for 60–90 seconds. Temperature and time can vary based on the nerve and clinical protocol.
Repeatability
Relief often lasts 6–12 months, with repeat RFA considered if pain recurs.
5.5 Shockwave Therapy Key Steps
Probe and Coupling
A handheld shockwave applicator is used with a coupling gel to ensure correct energy transmission.
Session Protocol
Typically 3–6 sessions, 1–2 weeks apart. Energy levels are gradually increased to patient tolerance.
Post-Treatment Advice
Some mild pain or bruising can occur; resting the treated area and light stretching may optimize recovery.
Written on December 22th, 2024
<
Clinical Guidance on Opioid and Adjunct Analgesics (Written December 22, 2024)
Opioid analgesics constitute a mainstay of therapy for moderate to severe pain. These agents include strong opioids such as morphine, fentanyl, oxycodone, hydromorphone, and moderate opioids such as tramadol (classified differently depending on local regulations). Certain combination products, such as Targin (oxycodone/naloxone), are designed to minimize opioid-related adverse effects, notably constipation.
Non-opioid analgesics (e.g., acetaminophen) remain valuable for mild pain or as adjuncts to opioid therapy, often providing synergistic pain relief and minimizing the required opioid dose. Careful assessment of pain severity, patient comorbidities, and risk factors for opioid misuse is essential when initiating and titrating any analgesic regimen.
Strong Opioids
Morphine
Fentanyl
Oxycodone (including combination products like Targin)
Hydromorphone
Norspan® (buprenorphine transdermal patch)
Moderate Opioids
Tramadol (classifications vary across regions)
Non-Opioid Analgesics
Acetaminophen
Medication
Indication
Contraindications
Side Effects
Typical Dosage & Duration
Common Brand Names
Pain Control (1–5)
Antidote
Other Important Aspects
Morphine (strong opioid)
Severe acute or chronic pain
Hypersensitivity
Severe respiratory depression
Acute asthma
Paralytic ileus
Nausea, vomiting
Constipation
Sedation
Pruritus
Respiratory depression
Oral (immediate-release): 15–30 mg every 4 hr PRN
IV: 2–10 mg every 2–4 hr PRN
Duration varies by clinical scenario; reassess regularly
MS Contin, Kadian
5
Naloxone (for overdose)
Considered the benchmark opioid
Monitor for sedation, respiratory status
May require opioid rotation if tolerance develops
Fentanyl (strong opioid)
Severe chronic pain (transdermal)
Acute severe pain (IV)
Adjunct in anesthesia
Opioid-naïve patients (for patch)
Severe respiratory depression
Hypersensitivity
Dizziness
Bradycardia
Hypotension
Constipation
Respiratory depression
Transdermal patch (Duragesic): 12–100 mcg/hr, changed every 72 hr
IV (Sublimaze): 25–100 mcg bolus; frequency depends on analgesic response
Naloxone: Serves as the standard opioid receptor antagonist for the rapid reversal of opioid-induced respiratory depression. Intravenous, intramuscular, subcutaneous, and intranasal formulations are available.
Typical Dosing: 0.4–2 mg IV or IM for acute overdose; may repeat every 2–3 minutes as needed based on clinical response.
Duration: Often shorter than that of many opioids, necessitating repeated dosing or continuous infusion depending on the half-life of the ingested opioid.
Safe Prescribing and Monitoring
Initial Assessment: Evaluate pain severity, prior analgesic history, current medications, comorbid conditions (e.g., renal or hepatic impairment), and potential risk of opioid misuse.
Start Low, Titrate Slow: Particularly in opioid-naïve or older adults to reduce the risk of respiratory depression.
Concurrent Therapy: Use multimodal analgesia (e.g., combining opioids with acetaminophen or non-pharmacological methods) to enhance efficacy and minimize opioid dosage.
Monitoring:
Pain Relief: Adjust dose or frequency based on reported pain levels.
Sedation and Respiratory Rate: Vigilance is paramount to detect respiratory depression early.
Opioid-Induced Constipation: Prophylactic use of laxatives or other bowel regimens may be necessary.
Potential for Dependence: Assess regularly for signs of misuse or diversion, particularly with long-term use.
Practical Considerations for Clinical Use
Medication
Onset (Approx.)
Duration (Approx.)
Morphine (oral IR)
30–60 minutes
3–5 hours
Fentanyl (transdermal)
12–24 hours
72 hours (patch replacement)
Oxycodone (oral IR)
30–60 minutes
4–6 hours
Tramadol (oral IR)
30–60 minutes
4–6 hours
Targin (extended-release)
30–60 minutes
~12 hours
Norspan (buprenorphine patch)
~12–24 hours
7 days (patch replacement)
Acetaminophen (oral)
30–60 minutes
4–6 hours
Acute Pain: Short-course therapy (days to weeks) is typically sufficient; reassessment is critical to avoid unnecessary prolonged opioid use.
Chronic Pain: Requires ongoing risk-benefit analysis, possibly involving an interprofessional team (e.g., pain management specialists, pharmacists). Opioid rotation or tapering may be necessary in the context of tolerance or side effects.
References and Further Reading
Goodman & Gilman’s The Pharmacological Basis of Therapeutics.
World Health Organization (WHO) Guidelines for the Pharmacological and Radiotherapeutic Management of Cancer Pain in Adults and Adolescents.
Official Prescribing Information for each product (MS Contin, Duragesic, Targin, etc.).
Local regulations and protocols regarding controlled substances.
Written on December 22th, 2024
Trigger Point Injections (Written December 22, 2024)
Trigger Point Injections (TPI) are an interventional pain management technique aimed at alleviating myofascial pain by targeting palpable hyperirritable spots within skeletal muscle, known as trigger points. These trigger points often generate local tenderness and may refer pain to distant sites. When appropriately performed, TPI can serve both diagnostic and therapeutic purposes, offering significant symptom relief in acute and chronic musculoskeletal pain syndromes.
A careful review of each treatment’s pharmacodynamics, procedural protocols, and potential adverse effects informs responsible clinical decision-making. Imaging techniques—such as ultrasound or fluoroscopy—further enhance safety and accuracy, helping ensure optimal patient outcomes.
Definition and Pathophysiology
Trigger Points (TPs):
Discrete, focal, hyperirritable nodules found in taut bands of skeletal muscle or its associated fascia. They are frequently linked to repetitive strain, muscle overuse, or underlying structural/postural imbalances.
Pathophysiology:
Sustained muscle contraction or microtrauma can lead to local ischemia, increased metabolic demand, and accumulation of inflammatory mediators. This cycle promotes persistent nociceptive input, culminating in local and referred pain.
Position in the Spectrum of Pain Management
Musculoskeletal/Soft Tissue Intervention:
TPI lies under the umbrella of interventional pain management techniques that specifically address myofascial pain rather than joint, nerve, or bursal pathology.
Minimally Invasive and Diagnostic:
Similar to other local injection therapies (e.g., nerve blocks, joint injections), TPI is minimally invasive. However, it is distinct in that it primarily focuses on muscular pain generators rather than nerves or joint capsules. If pain subsides after a TPI, the procedure helps confirm that specific muscle or trigger point as a primary contributor to the patient’s discomfort.
Comparison with Other Treatment Modalities
Modalities
Target Tissues
Primary Mechanism
Diagnostic / Therapeutic
Typical Injectate Components
Trigger Point Injections (TPI)
Myofascial trigger points
Disruption of localized spasm; sedation of nociceptors
Mechanism:
Unlike nerve blocks that halt conduction along a nerve, TPI reduces localized muscle hyperactivity and potential peripheral nerve irritation within that muscle.
Injectate Components:
May include only local anesthetics (e.g., lidocaine) or a combination of local anesthetic and a small dose of corticosteroid (e.g., triamcinolone, dexamethasone). In contrast to joint injections, TPI typically involves lower steroid doses—or none at all.
Medications Used in TPI
Medication
Mechanism
Typical Concentration / Dose
Key Points
Lidocaine (1% or 2%)
Sodium channel blockade; temporary analgesia
1–2 mL per trigger point
Common choice for diagnostic and therapeutic TPI; rapid onset, short to moderate duration
Bupivacaine (0.25–0.5%)
Sodium channel blockade; longer-acting local anesthetic
1–2 mL per trigger point
Longer analgesic duration than lidocaine; slow onset; caution for cardiotoxicity if inadvertent intravascular injection
Triamcinolone (“Triam”)
Anti-inflammatory corticosteroid
2–10 mg per injection (optional)
Added if a more prolonged anti-inflammatory effect is desired; excessive or frequent use can lead to tissue atrophy and other steroid-related side effects
Dexamethasone (“Dexa”)
Anti-inflammatory corticosteroid with high potency
0.5–2 mg per injection (optional)
Often used in low dose for longer-lasting anti-inflammatory effect; less risk of particulate-related complications
Normal Saline
Provides mechanical disruption of trigger point; no pharmacologic action
1–2 mL if anesthetic is contraindicated
Sometimes used in “dry needling with saline” to mechanically irritate and break up taut band without using local anesthetic or steroid
Indications and Contraindications
Indications
Myofascial Pain Syndrome (MPS):
Particularly where palpation reveals well-defined trigger points producing local or referred pain.
Chronic Musculoskeletal Pain:
When conservative measures (e.g., physical therapy, medications) have not yielded sufficient relief.
Diagnostic Confirmation:
To ascertain the extent of muscular involvement in complex pain syndromes.
Contraindications
Local Infection or Inflammation:
Infection at the injection site (abscess, cellulitis) or severely inflamed overlying skin.
Allergy to Injectate Components:
Known hypersensitivity to amide local anesthetics or corticosteroids.
Uncontrolled Bleeding Diathesis:
Significant coagulopathy or anticoagulant therapy that increases the risk of bleeding within muscle.
Pregnancy (Relative):
Most local anesthetics are category B or C. While TPI is not absolutely contraindicated, thorough risk-benefit consideration is advised.
Procedure and Technique
Patient Assessment and Preparation
Perform thorough history and physical examination to identify the most relevant trigger points.
Clean the injection area with appropriate antiseptic solution (e.g., chlorhexidine or povidone-iodine).
Identification of Trigger Points
Palpate for taut bands or nodules within the muscle. A characteristic “jump sign” or referred pain pattern often confirms trigger point location.
Needle Insertion
Use a small-gauge needle (often 25–27 G) to minimize discomfort.
Insert the needle into the trigger point, confirming a local twitch response if possible.
Injectate Administration
Inject 1–2 mL of chosen agent (e.g., 1% lidocaine ± small-dose corticosteroid).
Some protocols employ multiple passes (“peppering technique”) to ensure adequate distribution within the trigger area.
Aftercare and Monitoring
Gently stretch the involved muscle post-injection to help reduce residual tension.
Observe for any immediate adverse reactions (e.g., vasovagal response, allergic reaction).
Advise continuation of physical therapy and exercises to promote long-term improvement.
Potential Complications
Pain or Bruising at Injection Site:
Minor discomfort or hematoma may occur.
Infection:
Rare if proper aseptic technique is used.
Nerve or Vascular Injury:
Uncommon, provided the muscle group is accurately identified and the needle is appropriately sized.
Allergic Reactions:
Rare with amide local anesthetics, slightly higher risk if using ester-type or if patient is sensitive to preservatives.
Excessive Steroid Use Complications:
Tissue atrophy, local depigmentation, or systemic steroid effects if repeatedly administered in high doses.
Clinical Pearls and Conclusion
Integration with Physical Therapy:
Combining TPI with stretching, posture correction, and strengthening exercises yields better long-term outcomes.
Diagnostic Value:
A marked reduction in pain post-injection supports the diagnosis of myofascial trigger points contributing significantly to symptoms.
Minimal Steroid Requirement:
Trigger points often respond well to local anesthetic alone or even dry needling, limiting the need for frequent steroid use.
Distinguishing from Other Modalities:
TPI is unique in targeting muscular trigger points, whereas joint injections address articular pathology and nerve blocks focus on peripheral nerves.
Written on December 22th, 2024
Understanding the 0-10 Scale for NRS, FPS, and FLACC (Written April 8, 2025)
Pain assessment tools such as the Numeric Rating Scale (NRS), Faces Pain Scale (FPS), and FLACC (Face, Legs, Activity, Cry, Consolability) are used to quantify pain in different patient populations. Despite all ranging from 0 to 10 in their final scores, each tool has unique evaluation methods and interpretations. The table below provides a general guideline for each score level and how it can be identified.
1. Overview of Each Scale
NRS (Numeric Rating Scale): Patients verbally report a number from 0 to 10 based on their perceived pain intensity.
FPS (Faces Pain Scale): Patients, often children or individuals with limited verbal communication, select a facial expression that corresponds to their pain level. Although the classic FPS uses specific increments (e.g., 0, 2, 4, 6, 8, 10), it can be broadly mapped onto a 0–10 scale.
FLACC (Face, Legs, Activity, Cry, Consolability): An observer rates five categories (face, legs, activity, cry, consolability) from 0 to 2 points each, resulting in a total score between 0 and 10. It is useful for patients who cannot communicate verbally.
2. Score Interpretation Table (0–10)
Score
NRS
FPS
FLACC
How to Identify
0
No pain
No pain (Neutral face)
Relaxed and comfortable; no evident pain behaviors
Persistent cry, kicking or tense legs, restless activity, difficult to console
Observe intense pain expressions; patient may be unable to rest or focus.
8
Severe to very severe pain
Very severe pain (Crying face, tears, possibly clenched facial muscles)
Marked facial grimace, legs drawn up, vigorous crying, very limited consolability
High distress with continuous crying, increased agitation or fear.
9
Very severe pain
Very severe pain (Strong cry, extreme upset or anguish in face)
Almost inconsolable crying, rigid body posture or flailing, severe discomfort
Pain is nearly overwhelming; requires urgent attention.
10
Worst possible pain
Worst pain (Crying or screaming face indicating unbearable pain)
Totally inconsolable, may appear rigid or thrashing, extreme distress in all categories
Maximum distress, patient or observer indicates unbearable pain.
3. Practical Application
Choose the Appropriate Tool
NRS for verbally communicative adults or older children.
FPS for young children or those who respond best to visual aids.
FLACC for infants, very young children, or those unable to self-report pain.
Evaluate in Context
Pain scores should be interpreted alongside clinical observations, patient history, and other vital signs.
Monitor Changes Over Time
A single score is less meaningful than a pattern of scores over time, especially when assessing response to treatment.
By systematically applying and interpreting the NRS, FPS, and FLACC scales, healthcare providers can more effectively manage pain across diverse patient populations, ultimately enhancing patient comfort and treatment outcomes.
Pain assessment tools are crucial for effective pain management and treatment outcomes by integrating standardized evaluation methods into clinical practice.
Written on April 8, 2025
1. 각 척도의 개요
NRS (Numeric Rating Scale, 숫자통증척도): 환자가 느끼는 통증 강도를 0부터 10까지 숫자로 직접 보고한다.
FPS (Faces Pain Scale, 얼굴통증척도): 언어적 소통이 어려운 어린이나 노인 환자가 표정 그림을 보고 본인의 통증 정도를 선택한다. 전형적으로 0, 2, 4, 6, 8, 10점을 사용하지만, 편의상 0~10점 체계로 확장하여 해석하기도 한다.
FLACC (Face, Legs, Activity, Cry, Consolability): 얼굴, 다리, 활동, 울음, 위로 가능성 등 5가지 항목을 각각 0~2점으로 평가하여 합산(총 0~10점)한다. 의사소통이 어려운 영유아나 인지장애 환자에게 적용된다.
2. 점수별 해석 표 (0~10)
점수
NRS
FPS
FLACC
파악 방법
0
통증 없음
통증 없음 (무표정)
편안하고 긴장 없는 상태; 통증 행동이 전혀 보이지 않음
NRS: 환자가 0점 보고; FPS: 무표정 얼굴 선택; FLACC: 모든 항목 0점
1
매우 약한 통증
약한 불편감 (아주 약간 찡그린 표정)
다리·얼굴에 가벼운 긴장, 미미한 활동 변화
관찰 시 가벼운 초조함; 환자는 “약간 아프다”라고 표현할 수 있음
2
경증 통증
약간의 통증 (조금 걱정스러운 표정)
얼굴·다리에 약간의 긴장, 활동이 소폭 감소
미세한 표정 변화나 약한 짜증을 포착; 아동은 약간 아픈 표정을 선택할 수 있음
3
경증에서 중등도에 가까운 통증
경증에서 중등도 통증 (걱정되거나 살짝 괴로워 보이는 얼굴)
뚜렷하지 않지만 주기적인 찡그림, 간헐적 울음 또는 보챔
집중력이 다소 떨어지지만 일상 활동은 유지; 통증 호소는 분명함
4
중등도 통증
중등도 통증 (눈에 띄게 불편해 보이는 얼굴)
간헐적 울음, 보호적 행동, 불편감이 명확함
환자: 통증 호소 증가; 관찰자: 명확한 통증 행동(얼굴 찌푸림 등) 확인
5
중등도로 일상 활동에 일부 지장 있을 수 있는 통증
약간 심한 통증 (통증으로 인해 고통스러워 보이는 얼굴)
주기적으로 심한 울음, 때때로 강한 울음 또는 신음; 부분적 위로 시 일시적 완화
중간 정도 이상의 통증으로 활동 제한; FPS에서는 심각해 보이는 얼굴 선택 가능
6
중등도에서 심각해지는 통증
꽤 고통스러운 표정 (울거나 매우 괴로워 보임)
자주 울고, 안절부절, 다리를 끌거나 보호적 반응
통증 완화를 요구; 얼굴과 행동에서 강한 통증 징후가 나타남
7
심한 통증
심한 통증 (우는 표정, 눈물 보임 등)
끊임없이 울고, 다리를 구부리거나 신체부림이 심함; 위로가 어려움
격렬한 통증 반응; 환자가 휴식이나 집중 어려움
8
매우 심한 통증
매우 심한 통증 (울음, 일그러진 얼굴, 근육 경직 가능)
강한 찡그림, 다리 모으기, 격렬한 울음, 거의 위로 불가능
극심한 통증 상태; 지속적인 울음과 불안정한 움직임
9
극심한 통증
극심한 통증 (거의 울부짖는 표정, 극도로 힘들어 보임)
달래기 어려울 정도로 울고, 몸이 뻣뻣하거나 마구 움직임
환자가 극심한 고통을 호소; 즉각적 중재 필요
10
상상할 수 있는 가장 극심한 통증
참을 수 없는 통증 (절규 혹은 비명을 지르는 표정)
완전히 달래지지 않고, 몸이 경직되거나 격렬하게 움직이며 극도의 불안정 상태
최고 수준의 통증 고통; 즉각적인 통증 관리 필요
3. 임상에서의 활용
환자 특성에 맞는 척도 선택
언어 소통이 가능한 성인 및 아동: NRS
어린이나 시각적 이해가 더 쉬운 대상: FPS
영유아·인지장애로 자가 보고 어려운 환자: FLACC
상황과 함께 해석
통증 점수만으로는 한계가 있으므로, 환자의 전반적 임상 상태, 활력 징후, 과거 병력 등을 종합적으로 고려한다.
경과 관찰의 중요성
한 번의 측정 결과보다 시간이 지남에 따라 변화하는 통증 점수를 추적하여 치료나 중재 효과를 평가한다.
통증 평가 도구를 체계적으로 적용하고 해석함으로써, 다양한 환자군에서 통증 관리를 보다 효과적으로 수행할 수 있으며, 이는 환자의 편안함과 치료 성과를 높이는 데 도움이 될 것이다.
정확하고 일관된 통증 평가를 통해 임상 실무에서 보다 효과적인 통증 관리가 이루어질 수 있다.
Clinical Protocols and Intervention Procedures
Locking and Unlocking Pigtail Catheters
Pigtail catheters, commonly used for fluid drainage from various body cavities, employ unique locking mechanisms to maintain secure positioning. Proper handling of these mechanisms ensures both effective drainage and safe removal. This guide outlines the process for preparing a catheter for locking and removal, followed by detailed descriptions of locking and unlocking techniques for different types of catheters from brands such as Boston®, Cook®, Sung Won®, as well as additional designs that include manual release tabs and balloon-end catheters.
Preparing for Pigtail Catheter Locking
Before locking a pigtail catheter into position:
Ensure Optimal Placement: Confirm the catheter’s tip is correctly positioned within the target cavity, using imaging or clinical guidance.
Maintain Sterility: Establish a sterile field around the insertion site to minimize infection risk, employing sterile gloves, antiseptics, and proper dressing materials.
Activate the Locking Mechanism: Engage the catheter’s locking mechanism to create the pigtail shape, securing its position within the cavity.
Preparing for Pigtail Catheter Removal
Patient Preparation: Position the patient comfortably and provide a clear explanation of the removal procedure. Local anesthetic may be considered if the catheter has been in place for a prolonged period.
Maintain a Sterile Field: Ensure sterility around the removal site using gloves, antiseptic solutions, and sterile dressing supplies to prevent infection.
Release Tube Securing Mechanisms:
Suture Removal: Carefully cut and remove any sutures securing the catheter without causing irritation.
Adhesive Removal: For adhesive-secured catheters, gently peel the adhesive off, using an adhesive remover if necessary to avoid skin trauma.
Complete Drainage: Confirm that all fluid has been fully drained to avoid complications. Attaching a syringe to the catheter’s port can help remove any residual fluid, ensuring a clear pathway for removal.
Close the Drainage Path: Once drainage is complete, close the catheter’s port to prevent backflow, maintaining a controlled environment for removal.
Locking and Unlocking Mechanisms
Below are the main locking and unlocking systems for different pigtail catheter types, outlining each brand’s unique approach.
Boston® Pigtail Catheters
Locking: After the catheter is positioned, a gentle pull on the proximal ring or tab secures the distal end in a coiled configuration, anchoring it within the cavity.
Unlocking: To remove, pressing down or releasing the locking tab allows the pigtail to unwind gradually, creating a smooth pathway for extraction.
Cook® Pigtail Catheters
Locking: Once the catheter is placed, pulling the proximal ring activates the pigtail, securing it within the drainage site.
Unlocking: Gently disengaging the pull-ring releases the pigtail, allowing it to unfold gradually, minimizing resistance during withdrawal.
Sung Won® Pigtail Catheters
Locking: After insertion, a clockwise twist of the proximal end activates the pigtail shape, securing it in place.
Unlocking: A counterclockwise twist releases the lock, allowing the pigtail to straighten and enabling a gentle, smooth removal.
Manual Release Tabs
Locking: Pressing the tab after insertion locks the pigtail into place.
Unlocking: Releasing the tab allows the pigtail to uncoil naturally, providing a hands-on approach to catheter management.
Balloon-End Catheters
Locking: Inflating the balloon through the designated port after insertion keeps the catheter firmly in place.
Unlocking: Deflating the balloon via the inflation port releases the catheter, enabling it to be withdrawn gently.
Type
Locking Mechanism
Unlocking Mechanism
Benefits
Downsides
Boston®
Pull-lock with proximal ring or tab
Press or release locking tab
Provides reliable anchoring; smooth release
Requires manual release for unlocking
Cook®
Pull-ring at proximal end
Disengage pull-ring
Intuitive mechanism; low resistance on removal
Can feel rigid if not disengaged properly
Sung Won®
Twist-lock with clockwise rotation
Counterclockwise twist
Simple locking/unlocking; smooth transition
Risk of catheter resistance if not fully untwisted
Manual Release Tabs
Manual press-tab for locking/unlocking
Manual release of tab
Direct control over lock and release
Can be cumbersome in tight spaces
Balloon-End
Inflatable balloon at distal end
Deflate balloon via inflation port
Secure anchoring; low trauma on removal
Requires additional step to deflate balloon
This overview of locking and unlocking techniques provides a comprehensive guide to handling pigtail catheters from various brands, ensuring a secure yet gentle process tailored to each design for both effective drainage and patient comfort.
Written on November 4th, 2024
Differentiating Rhythms in Cardiac Arrest, for CPR and Defibrillation
In the management of cardiac arrest, swift recognition and differentiation of two primary categories of cardiac rhythms—shockable and non-shockable—are essential to ensure appropriate and effective intervention. Each rhythm type calls for specific actions that, when executed correctly, can be critical to patient survival.
Rhythm Category
Type of Rhythm
Description
Primary Intervention
Shockable
Ventricular Fibrillation (VF)
Chaotic, disorganized electrical activity in ventricles
Defibrillation
Pulseless Ventricular Tachycardia (VT)
Rapid, organized rhythm in ventricles, no pulse
Defibrillation
Non-Shockable
Asystole
Absence of electrical activity ("flatline")
CPR and medication
Pulseless Electrical Activity (PEA)
Electrical activity without effective heart contraction
CPR and address underlying causes
Shockable Rhythms
These rhythms respond to defibrillation, a procedure that delivers an electric shock to reset the heart’s rhythm. The two main types of shockable rhythms are:
Ventricular Fibrillation (VF)
Characterized by chaotic, erratic electrical impulses in the ventricles, VF prevents organized contraction and disrupts effective cardiac output. This disordered rhythm makes it impossible for the heart to pump blood adequately, requiring defibrillation to restore coordinated electrical activity.
Pulseless Ventricular Tachycardia (VT)
In this case, the ventricles display a rapid, organized rhythm, but there is no palpable pulse. The speed of this rhythm prevents proper filling of the heart, resulting in ineffective pumping and leading to cardiac arrest. Defibrillation is indicated to halt this arrhythmia and allow the heart’s natural pacemaker to re-establish a viable rhythm.
Immediate defibrillation is the primary intervention for shockable rhythms, as it interrupts the abnormal electrical activity and facilitates the heart's return to an organized rhythm.
Non-Shockable Rhythms
These rhythms do not benefit from defibrillation. Instead, management focuses on high-quality CPR to maintain circulation, along with targeted medical intervention. Non-shockable rhythms include:
Asystole
Known as "flatline," asystole signifies the complete absence of electrical activity in the heart. Because there is no activity to reset, defibrillation is ineffective. Immediate CPR and medication administration are the key responses.
Pulseless Electrical Activity (PEA)
This rhythm displays organized electrical activity on an ECG, but there is no corresponding mechanical contraction, resulting in no effective circulation. PEA requires CPR and urgent assessment to identify and address possible underlying causes, such as hypoxia, acidosis, or electrolyte imbalances.
For non-shockable rhythms, continuous CPR is essential, along with prompt treatment of reversible causes, to support cardiac function and improve the likelihood of restoring a viable rhythm.
Written on November 9th, 2024
Timing of epinephrine during CPR in cardiac arrest (Written December 30, 2025)
Appropriate timing of epinephrine administration during cardiopulmonary resuscitation (CPR)
is determined primarily by whether the cardiac arrest rhythm is shockable or non-shockable.
This distinction is central to Advanced Cardiac Life Support (ACLS) algorithms.
Core principle
Non-shockable rhythms require early epinephrine.
Shockable rhythms prioritize defibrillation first, with epinephrine introduced after initial shocks fail.
Diagram: epinephrine timing during CPR (workflow)
Interpretation: Non-shockable rhythms (PEA/asystole) receive epinephrine early during CPR once IV/IO access is available.
Shockable rhythms (VF/pulseless VT) prioritize defibrillation first; epinephrine is introduced after unsuccessful initial shocks.
Epinephrine timing by rhythm category
Rhythm category
Specific rhythm
Initial priority
Timing of epinephrine
Dose and interval
Non-shockable
Asystole
High-quality CPR
As soon as IV/IO access is established
1 mg IV/IO every 3–5 min
Non-shockable
PEA
High-quality CPR
As early as possible during CPR
1 mg IV/IO every 3–5 min
Shockable
VF
Defibrillation
After failure of 2 defibrillation attempts
1 mg IV/IO every 3–5 min
Shockable
Pulseless VT
Defibrillation
After failure of 2 defibrillation attempts
1 mg IV/IO every 3–5 min
Rationale (concise)
Non-shockable rhythms
Defibrillation is not beneficial in asystole and PEA.
Epinephrine supports coronary perfusion pressure during CPR via α-adrenergic vasoconstriction.
Operational focus: CPR first, epinephrine early.
Shockable rhythms
Defibrillation is the most effective immediate therapy for VF/pulseless VT.
Epinephrine is introduced after initial shocks fail, then repeated every 3–5 minutes.